Orforglipron is an oral non-peptide GLP-1 receptor agonist. This page compares Orforglipron to other agents in its class, including Semaglutide (Wegovy), Tirzepatide (Zepbound), and Liraglutide (Saxenda, Victoza). Its distinct oral, non-peptide formulation offers a different administration approach compared to many existing GLP-1 receptor agonists.
Orforglipron Alternatives: How It Compares to Other GLP-1 Receptor Agonists
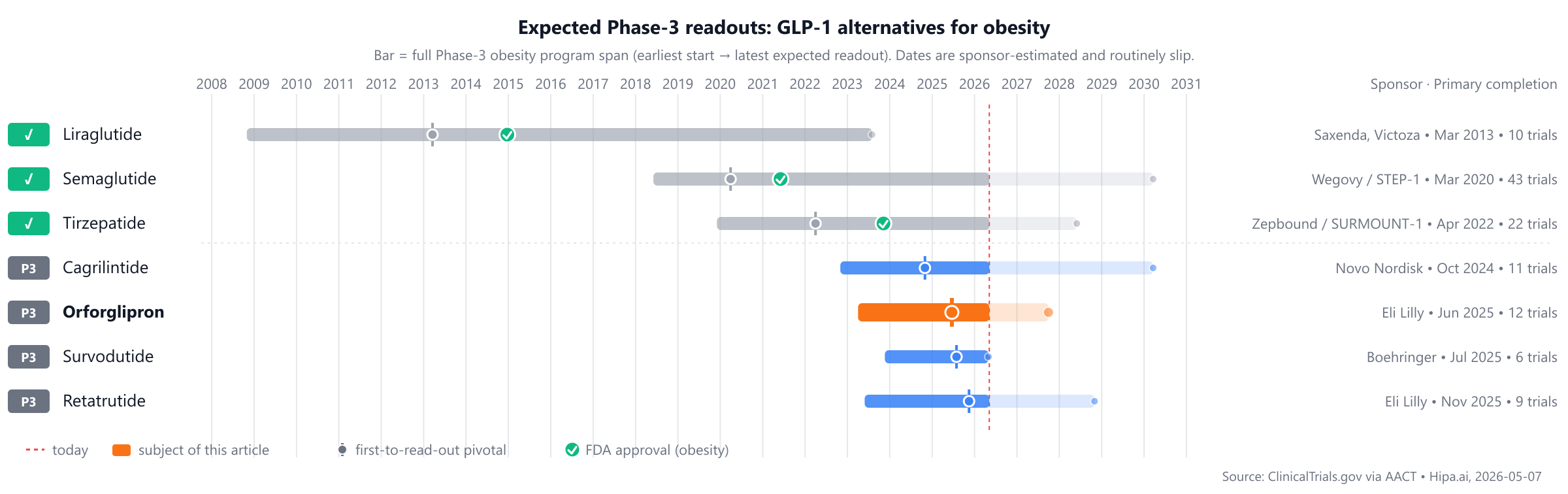
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: AI-augmented data · 5/7 curated
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape features established treatments such as Liraglutide (Saxenda, Victoza), approved in 2010, and Semaglutide (Wegovy), approved in 2017. While Orforglipron is a newer entrant, pipeline candidates like Retatrutide, Survodutide, and Cagrilintide are approximately 1-2 years behind in Phase 3 development.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Orforglipron | Oral non-peptide GLP-1 receptor agonist | — | Investigational; oral once-daily | Pipeline | — | — |
| Liraglutide (Saxenda, Victoza) | GLP-1 receptor agonist | type 2 diabetes, obesity, cardiovascular risk reduction | 3.0 mg once daily | 2014 | -7.46% @ 56 weeks | $16k |
| Semaglutide (Wegovy) | GLP-1 receptor agonist | chronic weight management, type-2 diabetes (Ozempic), cardiovascular risk reduction | 2.4 mg SC weekly (escalation from 0.25 mg over 16 weeks) | 2021 | -14.9% @ week 68 | $16k |
| Tirzepatide (Zepbound) | GIP/GLP-1 dual receptor agonist | chronic weight management, type-2 diabetes (Mounjaro), obstructive sleep apnea | 5–15 mg SC weekly (titration) | 2023 | -22.5% @ week 72 | $14k |
| Retatrutide | GLP-1/GIP/glucagon triple agonist | — | Investigational | Pipeline | — | — |
| Survodutide | GLP-1/glucagon dual agonist | — | Investigational | Pipeline | — | — |
| Cagrilintide | Amylin analogue | — | — | Pipeline | — | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Weight % change; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for obesity specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Orforglipron vs Semaglutide (Wegovy)
The pivotal head-to-head evidence comes from a head-to-head Phase-3 trial (NCT06045221) enrolling 1,698 participants, primary completion 2025-08.
Primary-endpoint values for NCT06045221 are not yet posted in the AACT results database.
Source: ClinicalTrials.gov via AACT — pulled directly from the trial's posted results. View the full trial record.
Orforglipron vs Tirzepatide (Zepbound)
No head-to-head Phase-3 trial directly compares Orforglipron with Tirzepatide.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Orforglipron vs Liraglutide (Saxenda, Victoza)
No head-to-head Phase-3 trial directly compares Orforglipron with Liraglutide.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Several investigational agents are currently in active Phase 3 development. Eli Lilly and Company is evaluating Retatrutide in a lead Phase 3 trial, NCT05931367. Boehringer Ingelheim is developing Survodutide, with its lead Phase 3 trial identified as NCT06214741. Additionally, Novo Nordisk A/S is advancing Cagrilintide, which has a lead Phase 3 trial listed under NCT05567796.
Choosing between Orforglipron and its alternatives
Orforglipron, an oral non-peptide GLP-1 receptor agonist, presents a distinct option for patients requiring weight management. Its oral formulation and once-daily dosing may offer a significant convenience advantage for individuals who prefer not to use injectable medications. This unique mechanism of action and administration route differentiates it from currently available injectable GLP-1 receptor agonists, potentially appealing to patients seeking a non-injectable therapeutic approach.
In contrast, established injectable GLP-1 receptor agonists offer different profiles. Semaglutide (Wegovy), administered subcutaneously once weekly, has demonstrated a mean weight change of -14.9% at week 68 in clinical trials. Tirzepatide (Zepbound), a dual GIP/GLP-1 receptor agonist, also administered weekly via subcutaneous injection, showed a mean weight change of -22.5% at week 72, potentially offering greater efficacy for some patients due to its dual mechanism. Liraglutide (Saxenda), a daily subcutaneous GLP-1 receptor agonist, demonstrated a mean weight change of -7.46% at 56 weeks. Clinicians may consider the longer track record and established safety profiles of these agents, as well as potential differences in cost or specific patient comorbidities that might favor a particular mechanism or administration schedule.
Ultimately, the choice of therapy is a complex clinical decision that should be made by the prescriber in consultation with the patient, considering individual patient characteristics, preferences, and clinical goals.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Head-to-head trials cited on this page:
- NCT06045221: Orforglipron vs Semaglutide · A Study of Orforglipron (LY3502970) Compared With Semaglutide in Participants With Type 2 Diabetes Inadequately Controll…
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
orforglipronorforglipron alternativesalternativescomparisonobesityorforglipron-glp1-obesityorforglipron vs semaglutideorforglipron vs tirzepatideorforglipron vs liraglutideorforglipron vs retatrutideorforglipron vs survodutide