Pelacarsen is an Antisense oligonucleotide. This page does not cover specific comparators for Pelacarsen within its class.
Pelacarsen Alternatives: How It Compares to Other Lp(a) Inhibitors
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: AI-augmented data · 0/4 curated
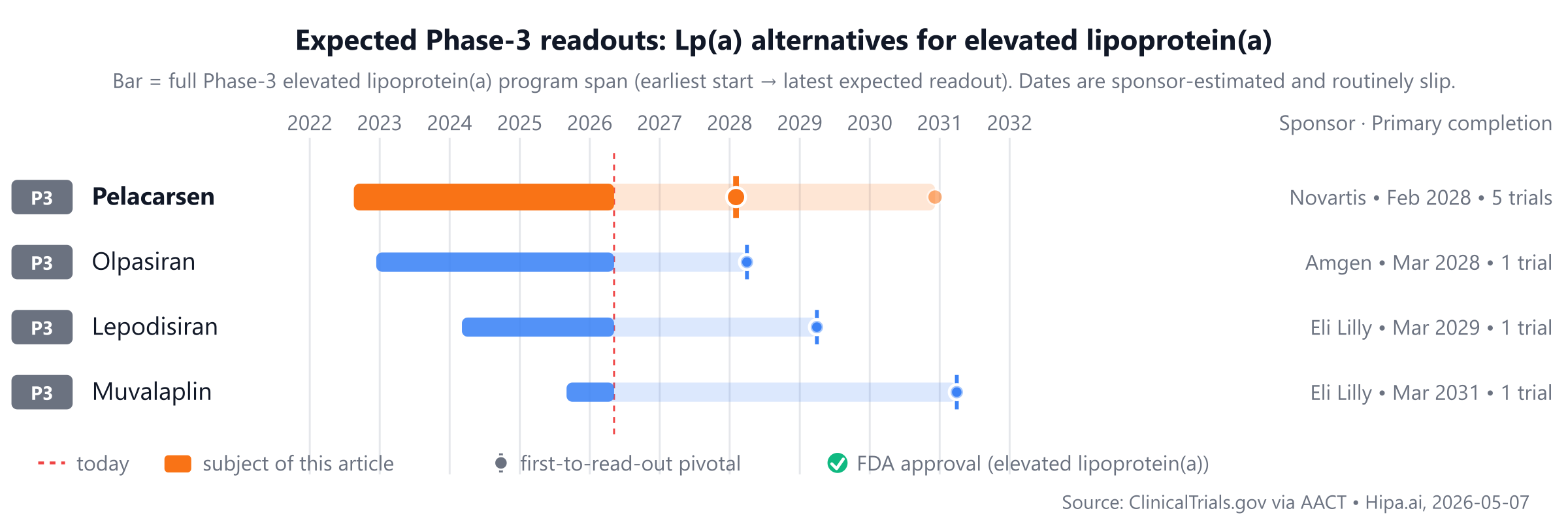
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
Pelacarsen is the sole approved comparator mentioned, while Olpasiran, Lepodisiran, and Muvalaplin are currently in Phase 3 development.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Pelacarsen | Antisense oligonucleotide | — | 80 mg subcutaneously once monthly | Pipeline | — | — |
| Olpasiran | Small interfering RNA (siRNA) | — | — | Pipeline | — | — |
| Lepodisiran | Small interfering RNA (siRNA) | — | Subcutaneous injection every 6 months | Pipeline | — | — |
| Muvalaplin | Lipoprotein(a) inhibitor | — | Oral, once daily | Pipeline | Lp(a) reduction: 85.8% @ 12 weeks | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Lp(a) % change; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for elevated lipoprotein(a) specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Pipeline alternatives
Several investigational agents are currently in active Phase 3 development. Among these is Olpasiran from Amgen, an siRNA agent, with its lead Phase 3 trial identified as NCT05581303. Eli Lilly and Company is developing Lepodisiran, also an siRNA agent, with its primary Phase 3 study designated NCT06292013. Also from Eli Lilly and Company, Muvalaplin is an oral small molecule, with its lead Phase 3 trial listed as NCT07157774. These agents represent different mechanistic approaches compared to Pelacarsen, which is an antisense oligonucleotide.
Choosing between Pelacarsen and its alternatives
Pelacarsen, as an antisense oligonucleotide, offers a highly specific mechanism for reducing lipoprotein(a) [lp(a)] levels. This targeted approach directly interferes with the production of lp(a), representing a distinct option for patients with elevated lp(a). Clinicians might consider Pelacarsen when a direct and potent reduction of lp(a) is the primary therapeutic goal, particularly in individuals with persistently high levels despite optimized conventional lipid-lowering therapies. Its novel mechanism could be a key factor in its selection for patients where other approaches are insufficient or contraindicated.
Alternatives to Pelacarsen may be considered based on factors such as established long-term safety data, which might be more extensive for therapies with a longer market presence. Cost-effectiveness could also play a role, as newer, targeted agents like Pelacarsen may have a higher initial price point compared to older medications. Furthermore, if a patient requires broader lipid management beyond lp(a) reduction, or has specific comorbidities that might benefit from a different pharmacological profile, an alternative agent with a different mechanism of action or a broader spectrum of effects might be preferred. Clinical decisions should always integrate individual patient characteristics, risk factors, and treatment goals.
This information is not medical advice; clinical decisions belong with the prescriber.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
pelacarsenpelacarsen alternativesalternativescomparisonelevated lipoprotein(a)lpa-elevated-lipoprotein-apelacarsen vs olpasiranpelacarsen vs lepodisiranpelacarsen vs muvalaplin