Camizestrant is a selective estrogen receptor degrader (SERD) being investigated for its role in hormone receptor-positive breast cancer. This page compares Camizestrant to other agents used in endocrine therapy, including the aromatase inhibitor Letrozole (Femara) and the investigational SERD Vepdegestrant (Veppanu). While all aim to disrupt estrogen signaling, Camizestrant and Vepdegestrant represent a distinct mechanism compared to aromatase inhibitors like Letrozole.
Camizestrant Alternatives: How It Compares to Other SERDs & Endocrine Therapies
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 0/8 curated
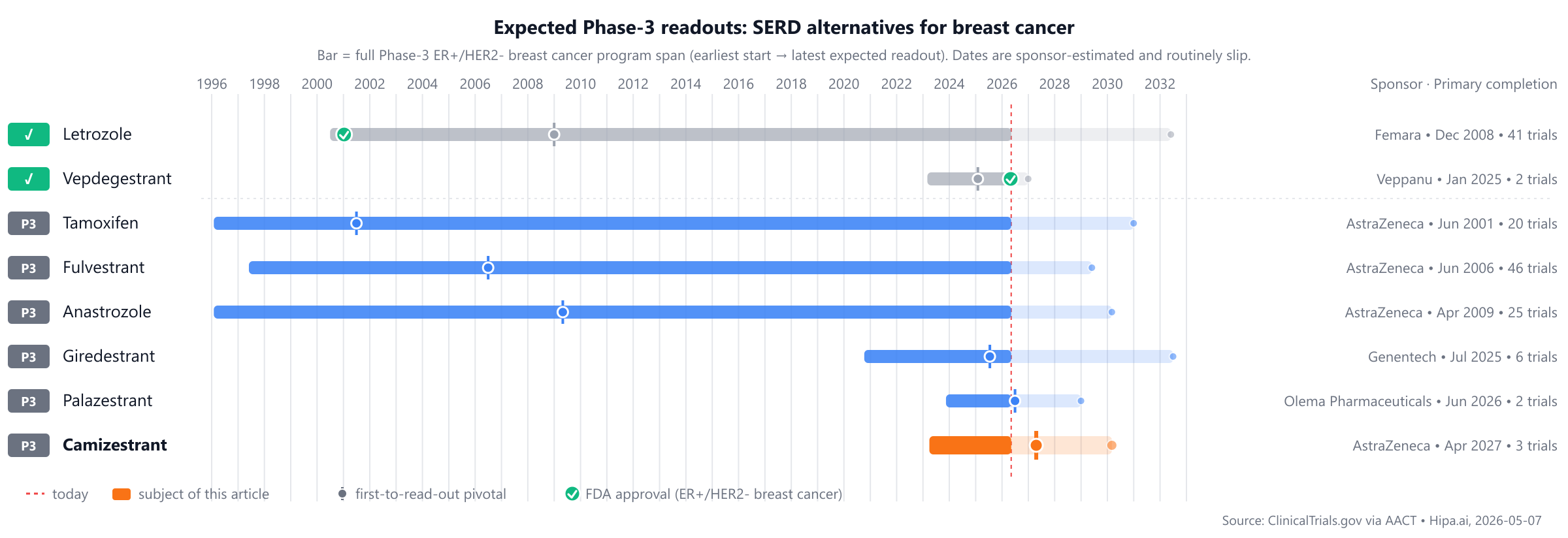
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape features approved comparators such as Femara (Letrozole), approved in 1997, and Veppanu (Vepdegestrant), approved in 2026. Camizestrant is not yet approved, while pipeline drugs including Fulvestrant, Tamoxifen, Anastrozole, Giredestrant, and Palazestrant are in Phase 3 development, estimated to be approximately 1-2 years behind.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Camizestrant | Selective estrogen receptor degrader | — | — | Pipeline | — | — |
| Letrozole (Femara) | Aromatase inhibitor | Advanced breast cancer, Early breast cancer, ER+/HER2- breast cancer | 2.5 mg once daily | 2001 | Disease-free survival (DFS): 84% @ 5 years | $150 |
| Vepdegestrant (Veppanu) | PROTAC estrogen receptor degrader | ESR1-mutated ER+/HER2- breast cancer | 200 mg orally once daily with food | 2026 | 5months @ Median | — |
| Fulvestrant | — | — | — | Pipeline | — | — |
| Tamoxifen | — | — | — | Pipeline | — | — |
| Anastrozole | — | — | — | Pipeline | — | — |
| Giredestrant | Selective estrogen receptor degrader | — | 30 mg orally once daily | Pipeline | 8.77months @ Median | — |
| Palazestrant | Complete estrogen receptor antagonist (CERAN) / Selective estrogen receptor degrader (SERD) | — | 90 mg once daily | Pipeline | — | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Progression-Free Survival (PFS); cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for ER+/HER2- breast cancer specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Camizestrant vs Letrozole (Femara)
The pivotal head-to-head evidence comes from a head-to-head Phase-3 trial (NCT05952557) enrolling 5,500 participants, primary completion 2030-03.
Primary-endpoint values for NCT05952557 are not yet posted in the AACT results database.
Source: ClinicalTrials.gov via AACT — pulled directly from the trial's posted results. View the full trial record.
Camizestrant vs Vepdegestrant (Veppanu)
No head-to-head Phase-3 trial directly compares Camizestrant with Vepdegestrant.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Several investigational alternatives are in active Phase 3 development, offering different mechanisms of action compared to Camizestrant, or representing next-generation oral selective estrogen receptor degraders (SERDs). Among these, established endocrine therapies include Fulvestrant from AstraZeneca, currently in a lead Phase 3 trial NCT00065325, Tamoxifen also from AstraZeneca in trial NCT00849030, and Anastrozole, another AstraZeneca agent, in trial NCT00256698. These agents represent current standards of care or well-established endocrine therapies.
In the realm of novel oral SERDs, similar to Camizestrant, are Giredestrant from Genentech, Inc., which is being investigated in a lead Phase 3 trial NCT05306340. Another oral SERD is Palazestrant from Olema Pharmaceuticals, Inc., with its lead Phase 3 study identified as NCT06016738. These oral SERDs are generally in a similar stage of development or slightly behind Camizestrant, aiming to provide oral alternatives to injectable SERDs like Fulvestrant.
Choosing between Camizestrant and its alternatives
Clinicians may consider Camizestrant, a selective estrogen receptor degrader (SERD), for its distinct mechanism of action. Unlike aromatase inhibitors such as Letrozole, SERDs directly degrade the estrogen receptor, which can be a crucial factor in managing hormone receptor-positive breast cancer, particularly in patients who may have developed resistance to other endocrine therapies. This targeted degradation approach offers a different strategy for inhibiting estrogen signaling.
Conversely, other endocrine therapies offer different profiles. Letrozole (Femara), an aromatase inhibitor, has a well-established track record, demonstrating disease-free survival of 84% at 5 years in relevant studies. Its dosing regimen is a straightforward 2.5 mg once daily. Vepdegestrant (Veppanu), a PROTAC estrogen receptor degrader, represents another distinct mechanism. Clinical data for Vepdegestrant indicates a median progression-free survival of 5 months with a dosing of 200 mg orally once daily with food. The choice between these agents may depend on the patient's prior treatment history, specific disease characteristics, and the desired mechanism of action.
This information is intended for educational purposes and does not constitute medical advice; clinical decisions should always be made by a qualified prescriber in consultation with their patient.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Head-to-head trials cited on this page:
- NCT06380751: Camizestrant vs Fulvestrant · Saruparib (AZD5305) Plus Camizestrant Compared With CDK4/6 Inhibitor Plus Endocrine Therapy or Plus Camizestrant in HR-P…
- NCT05952557: Camizestrant vs Tamoxifen · An Adjuvant Endocrine-based Therapy Study of Camizestrant (AZD9833) in ER+/HER2- Early Breast Cancer (CAMBRIA-2)
- NCT05952557: Camizestrant vs Letrozole · An Adjuvant Endocrine-based Therapy Study of Camizestrant (AZD9833) in ER+/HER2- Early Breast Cancer (CAMBRIA-2)
- NCT05952557: Camizestrant vs Anastrozole · An Adjuvant Endocrine-based Therapy Study of Camizestrant (AZD9833) in ER+/HER2- Early Breast Cancer (CAMBRIA-2)
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
camizestrantcamizestrant alternativesalternativescomparisonER+/HER2- breast cancerserd-breast-cancercamizestrant vs fulvestrantcamizestrant vs tamoxifencamizestrant vs letrozolecamizestrant vs anastrozolecamizestrant vs giredestrant