Tenapanor is an NHE3 inhibitor approved for the treatment of Irritable Bowel Syndrome with Constipation (IBS-C) and hyperphosphatemia in chronic kidney disease patients on dialysis. This page compares Tenapanor to other phosphate binders including Sevelamer Carbonate (Renvela), Ferric-citrate (Auryxia), Lanthanum carbonate (Fosrenol), and Calcium Acetate (PhosLo). Tenapanor's dual indications highlight a broader therapeutic application beyond phosphate binding alone.
Tenapanor Alternatives: How It Compares to Other Phosphate-Lowering Therapies
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 1/8 curated
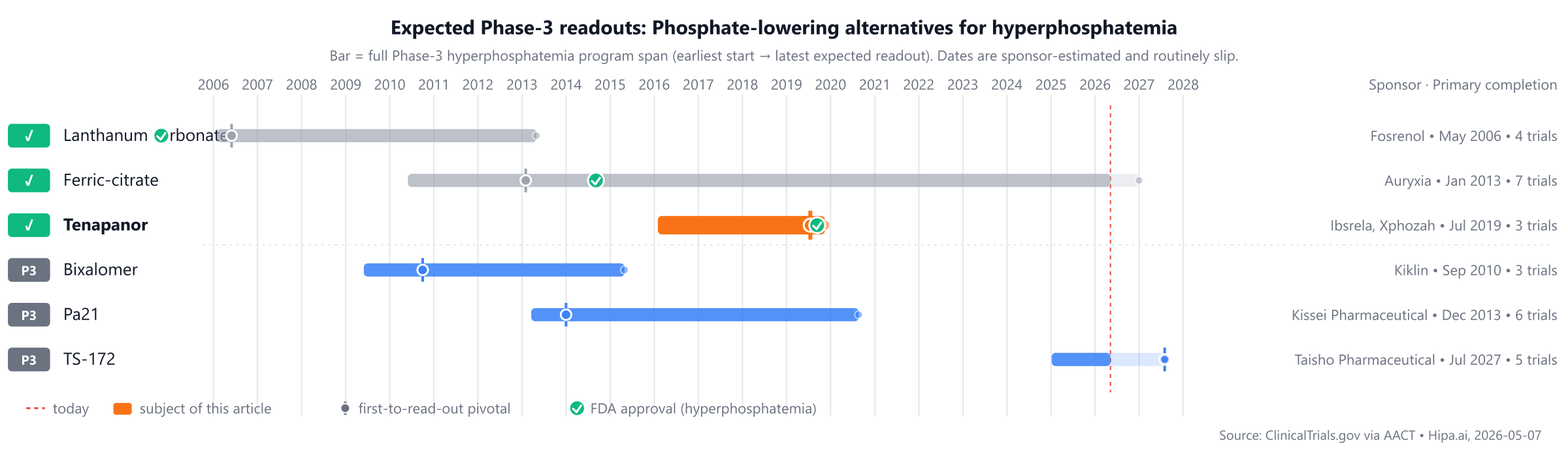
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape includes long-standing treatments such as Calcium Acetate (PhosLo, approved 1990) and Lanthanum carbonate (Fosrenol, approved 2004). Tenapanor was approved in 2019, while pipeline drugs Pa21, TS-172, and Bixalomer are still in Phase 3 development, potentially 1-2 years behind.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Tenapanor (Ibsrela, Xphozah) | NHE3 inhibitor | Irritable Bowel Syndrome with Constipation (IBS-C), Hyperphosphatemia in chronic kidney disease on dialysis | 50 mg twice daily for IBS-C; 30 mg twice daily for hyperphosphatemia | 2019 | Change in serum phosphorus: -0.84mg/dL @ Week 4 | $24k |
| Calcium Acetate (PhosLo) | Phosphate binder | hyperphosphatemia | 1334 mg (two 667 mg capsules/tablets) orally with each meal, titrated up to 3-4 capsules per meal as needed to control serum phosphorus | 1990 | — | — |
| Lanthanum carbonate (Fosrenol) | Phosphate binder | hyperphosphatemia in end-stage renal disease | 1500 mg to 3000 mg daily in divided doses with meals | 2004 | — | $15k |
| Sevelamer Carbonate (Renvela) | Phosphate binder | hyperphosphatemia | 0.8 to 1.6 g orally three times per day with meals; titrate by 0.8 g per meal at two-week intervals as needed | 2007 | — | $1k |
| Ferric-citrate (Auryxia) | Phosphate binder (iron-based) | hyperphosphatemia in CKD on dialysis, iron deficiency anemia in CKD not on dialysis | 2 tablets (210 mg ferric iron each) orally three times daily with meals; titrate up to max 12 tablets/day | 2014 | -2.04mg/dL @ 52 weeks | $14k |
| Pa21 | — | — | — | Pipeline | — | — |
| TS-172 | NHE3 inhibitor | — | — | Pipeline | — | — |
| Bixalomer (Kiklin) | Phosphate binder | — | 1500 mg to 7500 mg daily, administered orally in 3 divided doses just before meals | Pipeline | Change in serum phosphorus: -0.78mg/dL @ 12 weeks | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Serum phosphorus reduction; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for hyperphosphatemia specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Tenapanor vs Sevelamer Carbonate (Renvela)
No head-to-head Phase-3 trial directly compares Tenapanor with Sevelamer Carbonate.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Tenapanor vs Ferric-citrate (Auryxia)
No head-to-head Phase-3 trial directly compares Tenapanor with Ferric-citrate.
In separate pivotal trials, Tenapanor reported -0.84mg/dL Change in serum phosphorus at Week 4 (NCT03824587) versus -2.04mg/dL Serum phosphorus reduction at 52 weeks for Ferric-citrate (NCT01191255).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Tenapanor vs Lanthanum carbonate (Fosrenol)
No head-to-head Phase-3 trial directly compares Tenapanor with Lanthanum carbonate.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Tenapanor vs Calcium Acetate (PhosLo)
No head-to-head Phase-3 trial directly compares Tenapanor with Calcium Acetate.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Several investigational IL-17 / IL-17-related drugs are currently in active Phase 3 development, representing a different mechanistic approach compared to Tenapanor. Among these are Pa21 from Kissei Pharmaceutical Co., Ltd., with a lead Phase 3 trial NCT01850602; TS-172 from Taisho Pharmaceutical Co., Ltd., with a lead Phase 3 trial NCT07285304; and Bixalomer from Astellas Pharma Inc, with a lead Phase 3 trial NCT00892749. These agents are currently being evaluated in clinical trials as potential alternatives.
Choosing between Tenapanor and its alternatives
Tenapanor, an NHE3 inhibitor, offers a distinct mechanism of action for reducing serum phosphorus compared to traditional phosphate binders. While phosphate binders such as sevelamer carbonate, ferric citrate, lanthanum carbonate, and calcium acetate work by binding dietary phosphate in the gastrointestinal tract, tenapanor acts by inhibiting sodium-hydrogen exchanger 3 (NHE3), reducing paracellular phosphate absorption. This alternative approach may be considered for patients who do not achieve adequate phosphate control with binders alone or for those seeking a different therapeutic strategy.
Conversely, phosphate binders have a longer history of use in managing hyperphosphatemia. Ferric citrate, for example, has demonstrated a serum phosphorus reduction of -2.04 mg/dL at 52 weeks and may offer an additional benefit for patients with concomitant iron deficiency. Other binders like sevelamer carbonate, lanthanum carbonate, and calcium acetate are also widely used. Dosing for these binders typically involves administration with meals, often multiple times per day, such as 0.8 to 1.6 g of sevelamer carbonate three times daily, two tablets of ferric citrate three times daily, or 1500 mg to 3000 mg daily of lanthanum carbonate in divided doses. Calcium acetate is often dosed as two 667 mg capsules or tablets with each meal. Considerations for choosing a phosphate binder may include patient tolerance, pill burden, potential for calcium load with calcium acetate, or the desire to avoid specific elemental loads.
This information is for educational purposes only and does not constitute medical advice. Clinical decisions regarding patient care should always be made by a qualified healthcare provider.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
tenapanortenapanor alternativesalternativescomparisonhyperphosphatemiaphosphate-lowering-hyperphosphatemiatenapanor vs sevelamer carbonatetenapanor vs ferric-citratetenapanor vs lanthanum carbonatetenapanor vs pa21tenapanor vs calcium acetate