Seltorexant is an investigational Orexin-2 receptor antagonist. This page compares Seltorexant with Esketamine (Spravato), Duloxetine (Cymbalta), and Escitalopram (Lexapro). Its distinct mechanism of action targets specific sleep-wake pathways, differentiating it from other agents.
Seltorexant Alternatives: How It Compares to Other MDD Therapies
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 0/7 curated
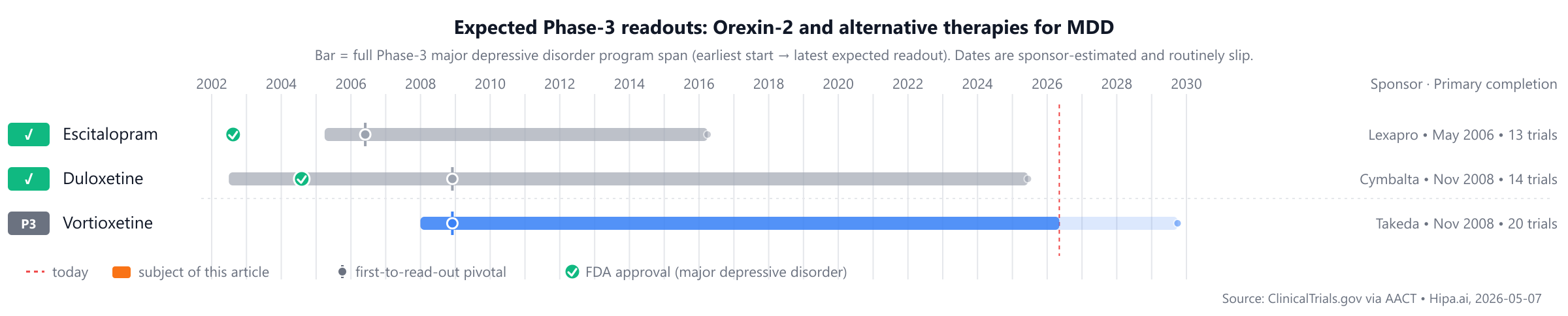
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape includes approved comparators such as Escitalopram (Lexapro) from 2002 and Duloxetine (Cymbalta) from 2004, while Seltorexant is not yet approved. Other pipeline drugs like Vortioxetine, Aticaprant, and Rapastinel are still in Phase 3, approximately 1-2 years behind.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Seltorexant | Orexin-2 receptor antagonist | — | 20 mg daily | Pipeline | Change in MADRS total score: -23points @ 26 weeks | — |
| Escitalopram (Lexapro) | Selective serotonin reuptake inhibitor | Major depressive disorder, Generalized anxiety disorder | 10 mg to 20 mg once daily | 2002 | — | $240 |
| Duloxetine (Cymbalta) | SNRI | Major depressive disorder, Diabetic peripheral neuropathic pain, Generalized anxiety disorder, +2 more | 40-60 mg/day | 2004 | — | $444 |
| Esketamine (Spravato) | NMDA receptor antagonist | Treatment-resistant depression, Depressive symptoms in adults with major depressive disorder with acute suicidal ideation or behavior | Induction (Weeks 1-4): 56 mg or 84 mg intranasally twice weekly. Maintenance (Weeks 5-8): 56 mg or 84 mg once weekly. Week 9 and thereafter: 56 mg or 84 mg once weekly or once every 2 weeks. | 2020 | — | $38k |
| Vortioxetine | — | — | — | Pipeline | — | — |
| Aticaprant | Kappa opioid receptor antagonist | — | — | Pipeline | — | — |
| Rapastinel | NMDA receptor modulator | — | — | Pipeline | — | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is MADRS score change; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for major depressive disorder specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Seltorexant vs Esketamine (Spravato)
No head-to-head Phase-3 trial directly compares Seltorexant with Esketamine.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Seltorexant vs Duloxetine (Cymbalta)
No head-to-head Phase-3 trial directly compares Seltorexant with Duloxetine.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Seltorexant vs Escitalopram (Lexapro)
No head-to-head Phase-3 trial directly compares Seltorexant with Escitalopram.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Several investigational agents are currently in active Phase 3 development. Among these is Vortioxetine from Takeda, with its lead Phase 3 trial identified as NCT00672620. Other compounds include Aticaprant and Rapastinel, for which sponsors are not specified. These investigational drugs are generally considered to be approximately 1-2 years behind the development timeline of Seltorexant.
Choosing between Seltorexant and its alternatives
Clinicians considering treatment options for major depressive disorder may weigh several factors when choosing between Seltorexant and other available therapies. Seltorexant, as an Orexin-2 receptor antagonist, represents a novel mechanism of action distinct from traditional antidepressants. This unique pharmacological approach may be a key consideration, particularly for patients who have not achieved an adequate response with agents targeting serotonin, norepinephrine, or NMDA receptors. The introduction of a new mechanism provides an additional avenue for therapeutic intervention in MDD management.
Conversely, established therapies such as duloxetine (an SNRI) and escitalopram (an SSRI) offer extensive clinical experience and may be available as lower-cost generic options, which can influence prescribing decisions. These agents have well-characterized safety and tolerability profiles that clinicians are familiar with. Esketamine (Spravato), an NMDA receptor antagonist, provides a distinct mechanism and administration route (intranasal, with dosing regimens of 56 mg or 84 mg twice weekly during induction, then weekly or bi-weekly for maintenance), which may be preferred in specific clinical contexts. The choice among these therapies often involves a careful assessment of a patient's individual history, tolerability to previous treatments, and specific clinical needs, balancing the potential benefits of a novel mechanism against the familiarity and cost-effectiveness of established options.
This information is for educational purposes only and does not constitute medical advice. Clinical decisions regarding patient care should always be made by a qualified healthcare professional.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
seltorexantseltorexant alternativesalternativescomparisonmajor depressive disorderorexin-2-mddseltorexant vs vortioxetineseltorexant vs esketamineseltorexant vs duloxetineseltorexant vs escitalopramseltorexant vs aticaprant