Olpasiran is a small interfering RNA (siRNA) that targets lipoprotein(a). This page compares Olpasiran with other lipid-lowering therapies, including Inclisiran (Leqvio), Alirocumab (Praluent), and Evolocumab (Repatha). These agents differ in their mechanisms of action and administration schedules.
Olpasiran Alternatives: How It Compares to Other Lp(a)-Lowering Therapies
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: AI-augmented data · 0/5 curated
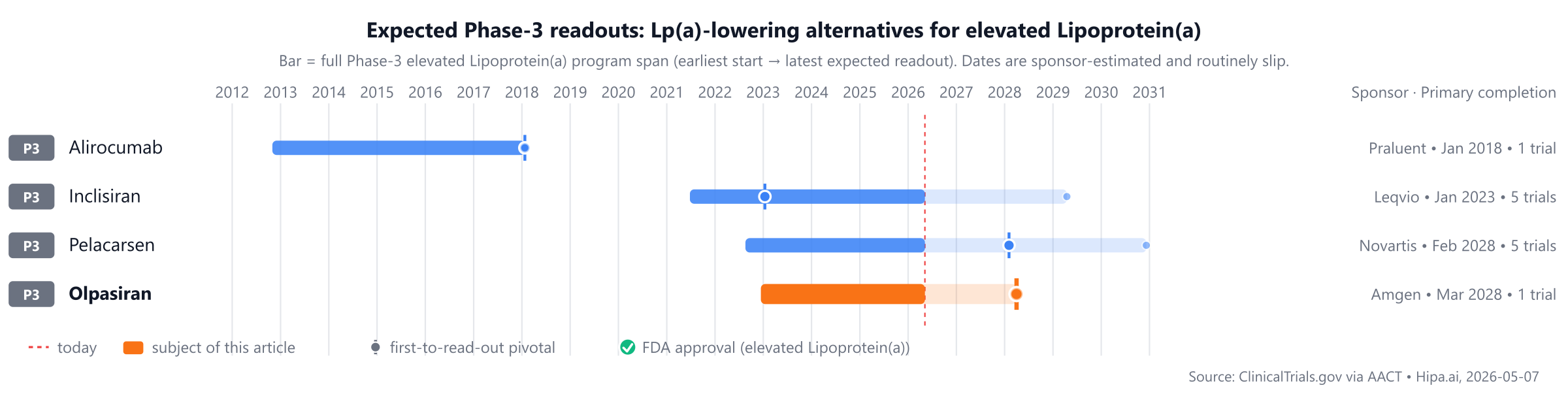
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape features established therapies such as Alirocumab (Praluent) and Evolocumab (Repatha), both approved in 2015, with Inclisiran (Leqvio) following in 2021. Olpasiran is not yet approved, placing it behind these established treatments, while other drugs like Pelacarsen are also in Phase 3 development, potentially 1-2 years from market entry.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Olpasiran | Small interfering RNA (siRNA) | — | — | Pipeline | — | — |
| Inclisiran (Leqvio) | PCSK9 inhibitor (siRNA) | high cholesterol, homozygous familial hypercholesterolemia | 284 mg subcutaneously initially, at 3 months, and then every 6 months | Pipeline | LDL-C reduction: 52.3% @ 17 months | $7k |
| Alirocumab (Praluent) | PCSK9 inhibitor | Heterozygous familial hypercholesterolemia, Clinical atherosclerotic cardiovascular disease, Prevention of cardiovascular events, +2 more | 75 mg or 150 mg subcutaneously once every 2 weeks, or 300 mg subcutaneously once every 4 weeks | Pipeline | — | $6k |
| Evolocumab (Repatha) | PCSK9 inhibitor | Primary hyperlipidemia, Homozygous familial hypercholesterolemia, Cardiovascular risk reduction | 140 mg every 2 weeks or 420 mg once monthly | Pipeline | — | $6k |
| Pelacarsen | Antisense oligonucleotide | — | 80 mg subcutaneously once monthly | Pipeline | — | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Lp(a) % reduction; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for elevated Lipoprotein(a) specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Olpasiran vs Inclisiran (Leqvio)
No head-to-head Phase-3 trial directly compares Olpasiran with Inclisiran.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Olpasiran vs Alirocumab (Praluent)
No head-to-head Phase-3 trial directly compares Olpasiran with Alirocumab.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Olpasiran vs Evolocumab (Repatha)
No head-to-head Phase-3 trial directly compares Olpasiran with Evolocumab.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Several investigational drugs are currently in active Phase 3 development. These include Inclisiran from Novartis, with its lead Phase 3 trial identified as NCT04807400. Alirocumab, developed by Sanofi, is also undergoing Phase 3 evaluation, with a lead trial designated NCT01663402. Evolocumab represents another investigational agent in this stage of development. Additionally, Novartis is advancing Pelacarsen, for which a lead Phase 3 trial is registered as NCT06813911.
Choosing between Olpasiran and its alternatives
Olpasiran, as a small interfering RNA (siRNA) therapy, represents a distinct approach for clinicians considering therapies specifically designed to lower lipoprotein(a) (Lp(a)). While other agents like Inclisiran, Alirocumab, and Evolocumab are also siRNA or monoclonal antibody therapies, their primary mechanism involves PCSK9 inhibition, leading predominantly to reductions in LDL-C. Therefore, Olpasiran may be a preferred option when the clinical objective is a targeted reduction of Lp(a), distinguishing it from therapies focused primarily on LDL-C management.
Conversely, for patients where significant LDL-C reduction is the primary goal, PCSK9 inhibitors offer established efficacy and various dosing schedules. Inclisiran (Leqvio), also an siRNA, has demonstrated an LDL-C reduction of 52.3% at 17 months with a convenient dosing regimen of 284 mg subcutaneously initially, at 3 months, and then every 6 months. Alirocumab (Praluent) and Evolocumab (Repatha) are other PCSK9 inhibitors providing flexible dosing options, such as 75 mg or 150 mg subcutaneously every 2 weeks, or 300 mg every 4 weeks for Alirocumab, and 140 mg every 2 weeks or 420 mg once monthly for Evolocumab. These agents may be considered based on their established role in LDL-C lowering and patient-specific dosing preferences.
This information is for educational purposes only and does not constitute medical advice; clinical decisions should always be made by a qualified prescriber in consultation with the patient.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
olpasiranolpasiran alternativesalternativescomparisonelevated Lipoprotein(a)olpasiran-lpa-elevated-lipoprotein-aolpasiran vs inclisiranolpasiran vs alirocumabolpasiran vs evolocumabolpasiran vs pelacarsen