Nerandomilast is a PDE4B inhibitor approved for the treatment of idiopathic pulmonary fibrosis and progressive pulmonary fibrosis. This page provides a comparison of Nerandomilast with other established therapies for these conditions, including Pirfenidone (Esbriet) and Nintedanib (Ofev).
Nerandomilast Alternatives: How It Compares to Other Anti-fibrotics
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 0/7 curated
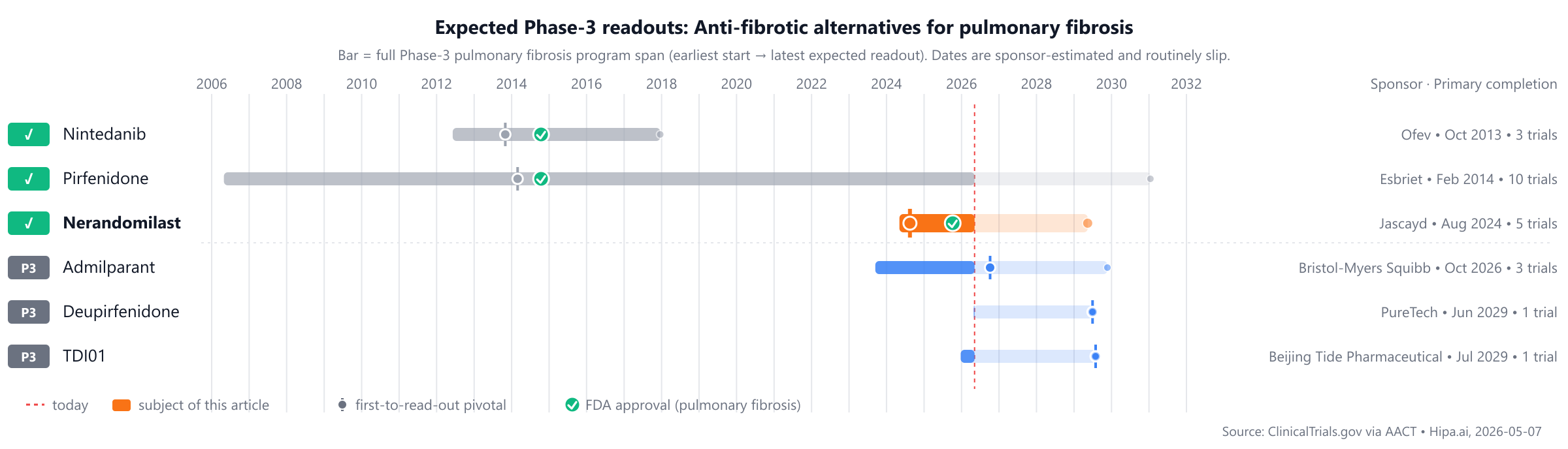
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
Pirfenidone (Esbriet) and Nintedanib (Ofev) were approved in 2014, preceding Nerandomilast's approval in 2025, with several other Phase 3 candidates like Inhaled-treprostinil, Admilparant, Deupirfenidone, and TDI01 trailing by approximately 1-2 years.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Nerandomilast (Jascayd) | PDE4B inhibitor | Idiopathic pulmonary fibrosis, Progressive pulmonary fibrosis | 18 mg twice daily | 2025 | Change in FVC: -114.7mL @ 52 weeks | — |
| Pirfenidone (Esbriet) | Anti-fibrotic agent | Idiopathic pulmonary fibrosis | 2403 mg/day (801 mg three times daily) with food | 2014 | Mean change in FVC: -235mL @ 52 weeks | $110k |
| Nintedanib (Ofev) | Tyrosine kinase inhibitor | pulmonary fibrosis, systemic sclerosis-associated interstitial lung disease, chronic fibrosing interstitial lung disease | 150 mg twice daily | 2014 | Annual rate of decline in FVC: -113.6mL/year @ 52 weeks | $100k |
| Inhaled-treprostinil | — | — | — | Pipeline | — | — |
| Admilparant | LPA1 antagonist | — | — | Pipeline | — | — |
| Deupirfenidone | Antifibrotic | — | — | Pipeline | — | — |
| TDI01 | ROCK2 inhibitor | — | — | Pipeline | FVC change vs placebo: 89mL @ 24 weeks | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is FVC decline; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for pulmonary fibrosis specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Nerandomilast vs Pirfenidone (Esbriet)
No head-to-head Phase-3 trial directly compares Nerandomilast with Pirfenidone.
In separate pivotal trials, Nerandomilast reported -114.7mL Change in FVC at 52 weeks (NCT05321069) versus -235mL Mean change in FVC at 52 weeks for Pirfenidone (NCT01366209).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Nerandomilast vs Nintedanib (Ofev)
No head-to-head Phase-3 trial directly compares Nerandomilast with Nintedanib.
In separate pivotal trials, Nerandomilast reported -114.7mL Change in FVC at 52 weeks (NCT05321069) versus -113.6mL/year Annual rate of decline in FVC at 52 weeks for Nintedanib (NCT01335464).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Several other investigational drugs are in active Phase 3 development. Admilparant, from Bristol-Myers Squibb, is an IL-17A nanobody with a different mechanism of action, currently being evaluated in a lead Phase 3 trial (NCT06003426). Beijing Tide Pharmaceutical Co., Ltd is developing TDI01, a PDE4 inhibitor, which is approximately 1-2 years behind Nerandomilast in development, with its lead Phase 3 trial listed as NCT07464912. PureTech is advancing Deupirfenidone, an antifibrotic agent with a distinct mechanism, in its lead Phase 3 study (NCT07284602).
Choosing between Nerandomilast and its alternatives
Nerandomilast, a PDE4B inhibitor, offers a distinct mechanism of action compared to established anti-fibrotics such as pirfenidone and nintedanib. This difference in pharmacological approach may be a primary consideration for clinicians exploring alternative therapeutic strategies, particularly for patients who may benefit from a pathway distinct from the general anti-fibrotic effects of pirfenidone or the tyrosine kinase inhibition of nintedanib. The introduction of a novel mechanism could expand treatment options for fibrotic conditions.
Conversely, established anti-fibrotic agents like pirfenidone (Esbriet) and nintedanib (Ofev) offer a longer track record of clinical use and well-characterized efficacy profiles. Pirfenidone, dosed at 2403 mg/day (801 mg three times daily with food), has shown a mean change in FVC of -235mL at 52 weeks. Nintedanib, administered at 150 mg twice daily, demonstrated an annual rate of decline in FVC of -113.6mL/year at 52 weeks. These agents may be preferred based on familiarity, extensive real-world experience, and their specific mechanisms of action, which are distinct from Nerandomilast. Clinicians might choose one of these established options based on their known efficacy in specific patient populations or their established safety and tolerability profiles.
This information is for comparative purposes only and does not constitute medical advice; clinical decisions should always be made by a qualified prescriber in consultation with their patient.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
nerandomilastnerandomilast alternativesalternativescomparisonpulmonary fibrosispde4b-pulmonary-fibrosisnerandomilast vs pirfenidonenerandomilast vs nintedanibnerandomilast vs inhaled-treprostinilnerandomilast vs admilparantnerandomilast vs deupirfenidone