Nemolizumab is an interleukin-31 (IL-31) receptor antagonist approved for the treatment of Prurigo Nodularis and Atopic Dermatitis. This page provides a comparison of Nemolizumab with other biologics used in the management of these conditions, highlighting differences in their mechanisms of action and approved indications.
Nemolizumab Alternatives: How It Compares to Other Biologics
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 0/5 curated
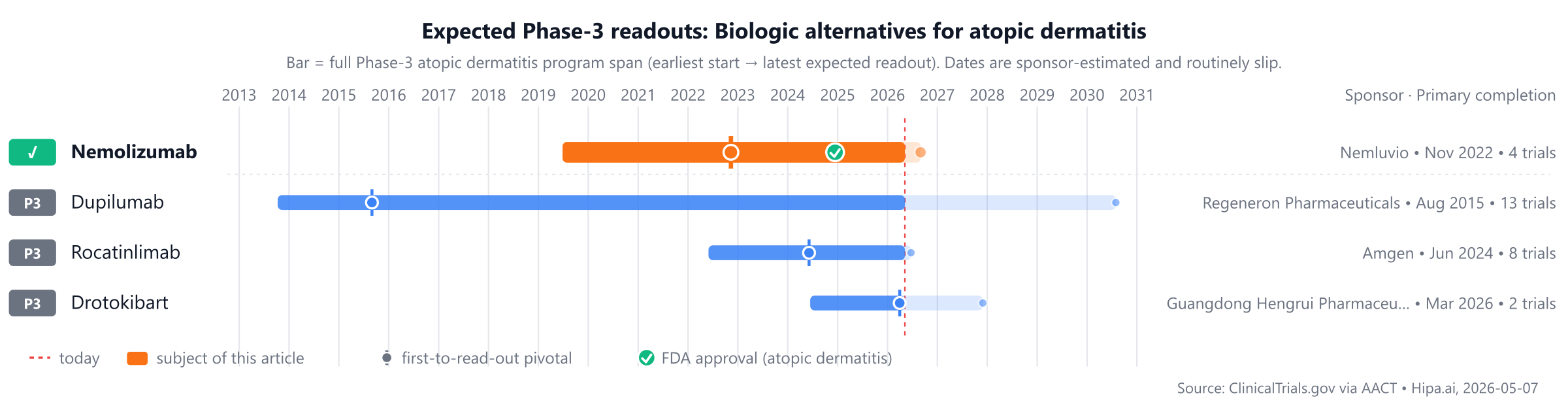
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
Among approved treatments, Nemolizumab was approved in 2024. Several pipeline drugs, including Dupilumab, Rocatinlimab, Drotokibart, and Stapokibart, are still in Phase 3, approximately 1-2 years behind.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Nemolizumab (Nemluvio) | IL-31 receptor antagonist | Prurigo Nodularis, Atopic Dermatitis | Initial dose of 60 mg SC (two 30 mg injections), followed by 30 mg or 60 mg SC every 4 weeks depending on body weight | 2024 | PP-NRS >= 4-point reduction: 49% @ 16 weeks | $57k |
| Dupilumab | — | — | — | Pipeline | — | — |
| Rocatinlimab | OX40 inhibitor | — | — | Pipeline | EASI-75: 42.3% @ 24 weeks | — |
| Drotokibart | IL-4Rα inhibitor | — | — | Pipeline | — | — |
| Stapokibart (Kangyueda) | IL-4Rα inhibitor | — | 600 mg initial dose, then 300 mg every 2 weeks | Pipeline | EASI-75: 66.9% @ 16 weeks | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is EASI 75; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for atopic dermatitis specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Pipeline alternatives
Investigational alternatives in active Phase 3 development include several agents with varying mechanisms of action. Dupilumab, from Regeneron Pharmaceuticals, is being investigated in a lead Phase 3 trial (NCT02260986), though its mechanism involves targeting the IL-4Rα subunit, distinct from direct IL-17 inhibition. Similarly, Rocatinlimab by Amgen, an anti-OX40 antibody, is also in Phase 3 development, with a lead trial NCT05651711, and is estimated to be approximately 1-2 years behind Nemolizumab in its development timeline.
Other investigational agents directly targeting IL-17 include Drotokibart from Guangdong Hengrui Pharmaceutical Co., Ltd, an IL-17A nanobody, with its lead Phase 3 trial NCT06468956. Another IL-17A nanobody, Stapokibart, is also in active Phase 3 development. Both Drotokibart and Stapokibart represent different mechanisms compared to Nemolizumab, specifically as IL-17A nanobodies.
Choosing between Nemolizumab and its alternatives
Nemolizumab, an interleukin-31 (IL-31) receptor antagonist, offers a distinct mechanism of action for conditions where IL-31 signaling is implicated. For patients whose disease is primarily driven by this specific pathway, nemolizumab may represent a targeted therapeutic option. Its unique approach could be particularly relevant in cases where other biologic mechanisms have not yielded optimal responses or are contraindicated, suggesting a potential role in patients with specific disease phenotypes.
Conversely, other biologics with longer clinical track records may be preferred for patients where extensive real-world experience is a priority, or when a different mechanism of action is deemed more appropriate for their specific disease characteristics. Cost considerations often play a significant role in treatment selection, and some established alternatives may offer a more favorable economic profile. Furthermore, the safety profiles of alternative biologics, which may differ from that of nemolizumab, could influence decisions for patients with specific comorbidities or risk factors.
Ultimately, the choice of therapy is a complex clinical decision that must be made by the prescriber in consultation with the patient, considering individual patient characteristics, disease severity, prior treatment history, and shared decision-making.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
nemolizumabnemolizumab alternativesalternativescomparisonatopic dermatitisil31-atopic-dermatitisnemolizumab vs dupilumabnemolizumab vs rocatinlimabnemolizumab vs drotokibartnemolizumab vs stapokibart