MM120 is a novel 5-HT2A receptor partial agonist. This page provides a comparison of MM120 with established antidepressants such as escitalopram (Lexapro), paroxetine (Paxil), and venlafaxine (Effexor). Understanding their distinct mechanisms of action is key for prescribers and patients.
MM120 Alternatives: How It Compares to Other Anxiolytics
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 0/5 curated
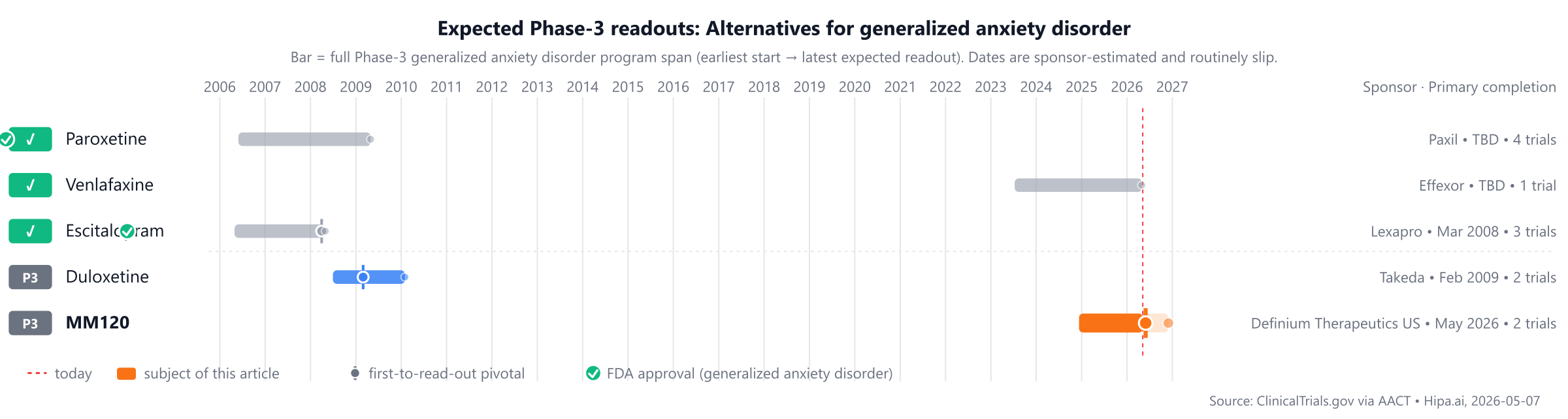
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape includes long-standing treatments such as Paroxetine (Paxil), approved in 1992, and Venlafaxine (Effexor), approved in 1993. While MM120 is not yet approved, Duloxetine is also in Phase 3 development, approximately 1-2 years behind the most recently approved comparators.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| MM120 | 5-HT2A receptor partial agonist | — | 100 µg single dose | Pipeline | 21.3points @ 4 weeks | — |
| Venlafaxine (Effexor) | Serotonin-norepinephrine reuptake inhibitor (SNRI) | major depressive disorder, generalized anxiety disorder, social anxiety disorder, +1 more | 37.5 mg to 225 mg orally once daily (extended-release) | 1999 | — | $350 |
| Paroxetine (Paxil) | Selective serotonin reuptake inhibitor | Major depressive disorder, Obsessive-compulsive disorder, Panic disorder, +5 more | 20 mg to 50 mg once daily | 2001 | — | — |
| Escitalopram (Lexapro) | Selective serotonin reuptake inhibitor | Major depressive disorder, Generalized anxiety disorder | 10 mg to 20 mg once daily | 2003 | — | $240 |
| Duloxetine | — | — | — | Pipeline | — | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is HAM-A reduction; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for generalized anxiety disorder specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
MM120 vs Escitalopram (Lexapro)
No head-to-head Phase-3 trial directly compares MM120 with Escitalopram.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
MM120 vs Paroxetine (Paxil)
No head-to-head Phase-3 trial directly compares MM120 with Paroxetine.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
MM120 vs Venlafaxine (Effexor)
No head-to-head Phase-3 trial directly compares MM120 with Venlafaxine.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Investigational alternatives in active Phase 3 development, based on the provided data, include duloxetine. Duloxetine, sponsored by Takeda, is currently being evaluated in a lead Phase 3 trial, NCT00730691. Duloxetine is a serotonin-norepinephrine reuptake inhibitor and is not an IL-17 or IL-17-related drug. The provided information does not include any IL-17 or IL-17-related therapies in active Phase 3 development. If MM120 is an IL-17-related therapy, duloxetine operates via a different mechanism of action.
Choosing between MM120 and its alternatives
MM120, a 5-HT2A receptor partial agonist, represents a distinct pharmacological approach to anxiolysis compared to selective serotonin reuptake inhibitors (SSRIs) such as escitalopram (Lexapro) and paroxetine (Paxil), or the serotonin-norepinephrine reuptake inhibitor (SNRI) venlafaxine (Effexor). This novel mechanism may be considered for patients seeking an alternative to traditional reuptake inhibitors, or when prior treatments targeting serotonin and norepinephrine reuptake have not been optimal.
Conversely, clinicians may opt for established agents like escitalopram, paroxetine, or venlafaxine due to their extensive clinical experience and generally lower cost, as many are available as generics. These SSRIs and SNRIs have well-characterized safety and tolerability profiles. Escitalopram is typically dosed at 10 mg to 20 mg once daily, while paroxetine ranges from 20 mg to 50 mg once daily. Venlafaxine extended-release offers a broader dosing range of 37.5 mg to 225 mg orally once daily, allowing for titration based on individual patient response and tolerability. The choice among these agents often depends on a patient's specific symptom profile, comorbidity, and prior treatment history.
Clinical decisions regarding anxiolytic treatment should always be made by a qualified prescriber, taking into account the individual patient's medical history, current medications, and specific therapeutic goals. This information is not medical advice.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
mm120mm120 alternativesalternativescomparisongeneralized anxiety disorder5-ht2a-generalized-anxietymm120 vs duloxetinemm120 vs escitaloprammm120 vs paroxetinemm120 vs venlafaxine