Lazertinib is an EGFR tyrosine kinase inhibitor approved for non-small cell lung cancer. This page compares Lazertinib with other agents in its class, including Osimertinib (Tagrisso), Erlotinib (Tarceva), and Gefitinib (Iressa). Key distinctions often relate to their specific binding profiles or efficacy against certain resistance mutations.
Lazertinib Alternatives: How It Compares to Other EGFR Inhibitors
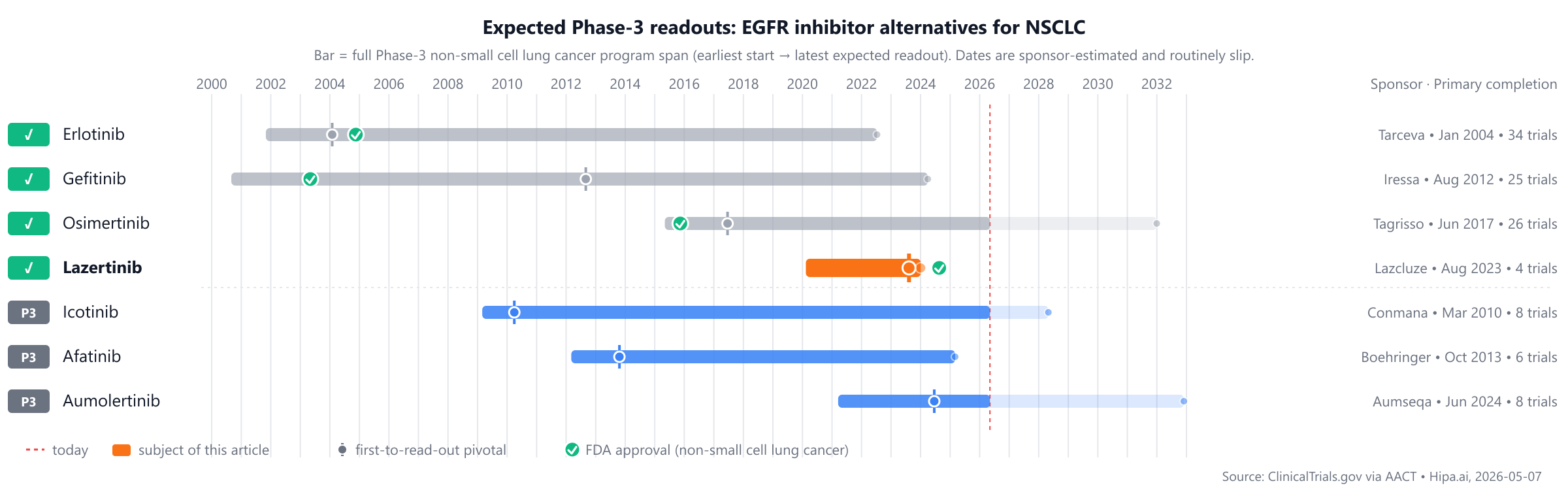
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 0/7 curated
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape includes long-standing approved treatments like Gefitinib (Iressa, 2003) and Erlotinib (Tarceva, 2004), with Lazertinib recently approved in 2024. Several other candidates, including Afatinib, Aumolertinib, and Icotinib, remain in Phase 3, potentially trailing by 1-2 years.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Lazertinib (Lazcluze) | EGFR tyrosine kinase inhibitor | Non-small cell lung cancer | 240 mg orally once daily | 2024 | PFS: 23.7months @ median | — |
| Gefitinib (Iressa) | EGFR tyrosine kinase inhibitor | non-small cell lung cancer | 250 mg orally once daily | 2003 | ORR: 69.8% @ overall | $70k |
| Erlotinib (Tarceva) | EGFR inhibitor | non-small cell lung cancer, pancreatic cancer | 150 mg orally once daily for non-small cell lung cancer; 100 mg orally once daily for pancreatic cancer | 2004 | OS: 6.7months @ median | — |
| Osimertinib (Tagrisso) | EGFR tyrosine kinase inhibitor | Metastatic EGFR T790M mutation-positive non-small cell lung cancer, First-line metastatic EGFR-mutated non-small cell lung cancer, Adjuvant treatment of early-stage EGFR-mutated non-small cell lung cancer, +2 more | 80 mg orally once daily | 2015 | 18.9months @ overall | $216k |
| Afatinib | — | — | — | Pipeline | — | — |
| Aumolertinib (Aumseqa) | EGFR tyrosine kinase inhibitor | — | 110 mg orally once daily | Pipeline | 19.3months @ median | — |
| Icotinib (Conmana) | EGFR tyrosine kinase inhibitor | — | 125 mg orally three times daily | Pipeline | — | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Progression-Free Survival; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for non-small cell lung cancer specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Lazertinib vs Osimertinib (Tagrisso)
The pivotal head-to-head evidence comes from a head-to-head Phase-3 trial (NCT04487080) enrolling 1,074 participants, primary completion 2023-08.
Progression-Free Survival (PFS) According to Response Evaluation Criteria in Solid Tumors (RECIST) Version 1.1 as Assessed by Blinded Independent Central Review (BICR): Active Comparator: Arm B (Double-blind): Osimertinib+Placebo Matching Lazertinib 16.59 Months; Experimental: Arm A (Open-label): Amivantamab + Lazertinib 23.72 Months; Experimental: Arm C (Double-blind): Lazertinib+Placebo Matching Osimertinib 18.46 Months
Source: ClinicalTrials.gov via AACT — pulled directly from the trial's posted results. View the full trial record.
Lazertinib vs Erlotinib (Tarceva)
No head-to-head Phase-3 trial directly compares Lazertinib with Erlotinib.
In separate pivotal trials, Lazertinib reported 23.7months PFS at median (NCT04487080) versus 6.7months OS at median for Erlotinib (NCT00036647).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Lazertinib vs Gefitinib (Iressa)
The pivotal head-to-head evidence comes from a head-to-head Phase-3 trial (NCT04248829) enrolling 393 participants, primary completion 2022-07.
Progression-Free Survival (PFS) According to RECIST v1.1 by Investigator Assessment: Gefitnib 250 mg 9.7 Months; Lazertinib 240 mg 20.6 Months
Source: ClinicalTrials.gov via AACT — pulled directly from the trial's posted results. View the full trial record.
Pipeline alternatives
Several investigational agents are in active Phase 3 development. These include Afatinib from Boehringer Ingelheim, with its lead Phase 3 trial NCT01523587. This agent is an earlier-generation EGFR TKI compared to Lazertinib. Aumolertinib, sponsored by Jiangsu Hansoh Pharmaceutical Co., Ltd., is also undergoing Phase 3 evaluation, with a key study NCT04923906. Aumolertinib shares a similar third-generation EGFR TKI mechanism with Lazertinib. Additionally, Icotinib from Betta Pharmaceuticals Co., Ltd. is in Phase 3 development, as exemplified by NCT01040780, representing another earlier-generation EGFR TKI.
Choosing between Lazertinib and its alternatives
Lazertinib is an EGFR tyrosine kinase inhibitor, a class of targeted therapies designed to inhibit tumor growth in specific patient populations. While specific comparative efficacy and safety data for Lazertinib are not detailed here, newer agents in this class are often developed with the aim of offering potential advantages such as improved efficacy, a more favorable safety profile, or convenient once-daily dosing. Clinicians considering Lazertinib would typically evaluate its profile based on available clinical trial data for specific patient characteristics and tumor mutations.
In contrast, other EGFR inhibitors offer established profiles. Osimertinib (Tagrisso) has demonstrated a median progression-free survival of 18.9 months and is dosed 80 mg orally once daily. Erlotinib (Tarceva) has a median overall survival of 6.7 months and is available for non-small cell lung cancer (150 mg orally once daily) and pancreatic cancer (100 mg orally once daily), offering a broader indication. Gefitinib (Iressa) has shown an overall response rate of 69.8% with a 250 mg orally once daily dose. These agents, with their longer track records and specific efficacy metrics, may be preferred based on factors such as established safety profiles, cost considerations, or specific indications like Erlotinib's use in pancreatic cancer.
Ultimately, the choice of EGFR inhibitor is a complex clinical decision that should be made by the prescriber in consultation with the patient, considering individual patient factors, tumor characteristics, and the full body of available evidence.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Head-to-head trials cited on this page:
- NCT04487080: Lazertinib vs Osimertinib · A Study of Amivantamab and Lazertinib Combination Therapy Versus Osimertinib in Locally Advanced or Metastatic Non-Small…
- NCT04248829: Lazertinib vs Gefitinib · Clinical Trial of YH25448(Lazertinib) as the First-line Treatment in Patients With EGFR Mutation Positive Locally Advanc…
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
lazertiniblazertinib alternativesalternativescomparisonnon-small cell lung canceregfr-nsclclazertinib vs osimertiniblazertinib vs afatiniblazertinib vs erlotiniblazertinib vs gefitiniblazertinib vs aumolertinib