Itepekimab is an investigational IL-33 inhibitor. This page compares its profile to Dupilumab (Dupixent), Ensifentrine (Ohtuvayre), Roflumilast (Daliresp, Zoryve), and Tiotropium (Spiriva). Its distinct mechanism of action as an IL-33 inhibitor offers a different therapeutic approach compared to these other agents.
Itepekimab Alternatives: How It Compares to Other IL-33 Inhibitors
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: AI-augmented data · 0/8 curated
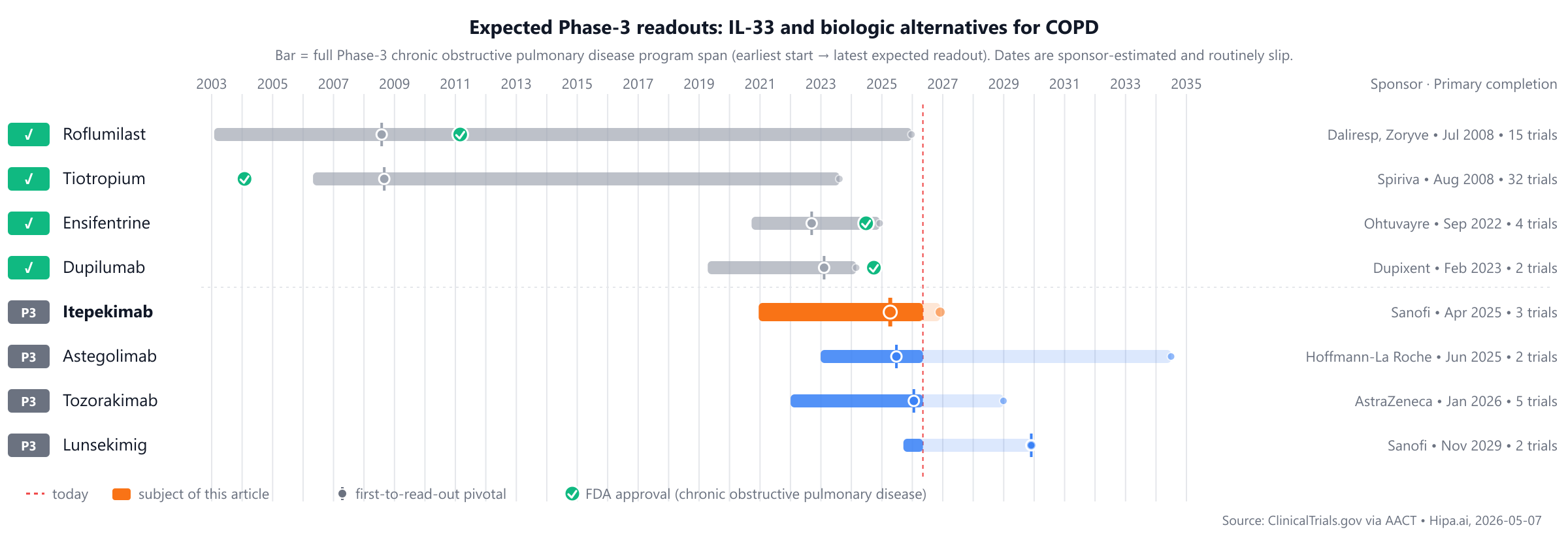
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape features long-standing treatments such as Tiotropium (Spiriva), approved in 2004, and Roflumilast (Daliresp, Zoryve) from 2011, alongside recent approval Ensifentrine (Ohtuvayre) in 2024. Itepekimab remains unapproved, while Tozorakimab, Astegolimab, and Lunsekimig are still in Phase 3 development.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Itepekimab | IL-33 inhibitor | — | 300 mg subcutaneously every 2 to 4 weeks | Pipeline | — | — |
| Tiotropium (Spiriva) | Long-acting muscarinic antagonist | Chronic obstructive pulmonary disease, Asthma | COPD: 18 mcg once daily via dry powder inhaler or 5 mcg once daily via inhalation spray. Asthma: 2.5 mcg once daily via inhalation spray. | 2004 | — | — |
| Roflumilast (Daliresp, Zoryve) | PDE4 inhibitor | chronic obstructive pulmonary disease, plaque psoriasis, seborrheic dermatitis, +1 more | 500 mcg orally once daily (COPD); applied topically once daily (dermatologic indications) | 2011 | reduction in moderate or severe exacerbations: 17% @ 52 weeks | $5k |
| Ensifentrine (Ohtuvayre) | Dual PDE3 and PDE4 inhibitor | chronic obstructive pulmonary disease | 3 mg twice daily via oral inhalation using a standard jet nebulizer | 2024 | change from baseline in FEV1 AUC0-12h: 87mL @ 12 weeks | $35k |
| Dupilumab (Dupixent) | IL-4 receptor alpha antagonist | atopic dermatitis, asthma, chronic rhinosinusitis with nasal polyps, +6 more | 300 mg subcutaneously every 2 weeks | 2024 | Reduction in annualized rate of moderate or severe exacerbations: 30% @ 52 weeks | $65k |
| Tozorakimab | IL-33 inhibitor | — | — | Pipeline | — | — |
| Astegolimab | ST2 inhibitor | — | — | Pipeline | — | — |
| Lunsekimig | TSLP and IL-13 inhibitor | — | — | Pipeline | — | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Annualized exacerbation rate; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for chronic obstructive pulmonary disease specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Itepekimab vs Dupilumab (Dupixent)
No head-to-head Phase-3 trial directly compares Itepekimab with Dupilumab.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Itepekimab vs Ensifentrine (Ohtuvayre)
No head-to-head Phase-3 trial directly compares Itepekimab with Ensifentrine.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Itepekimab vs Roflumilast (Daliresp, Zoryve)
No head-to-head Phase-3 trial directly compares Itepekimab with Roflumilast.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Itepekimab vs Tiotropium (Spiriva)
No head-to-head Phase-3 trial directly compares Itepekimab with Tiotropium.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Several investigational IL-17 / IL-17-related drugs are currently in active Phase 3 development. AstraZeneca is advancing Tozorakimab, with its lead Phase 3 trial registered as NCT05158387. Hoffmann-La Roche is developing Astegolimab, which is being investigated in a lead Phase 3 trial, NCT05595642. Additionally, Sanofi is progressing Lunsekimig, with its primary Phase 3 study identified as NCT07190222.
Choosing between Itepekimab and its alternatives
Itepekimab, as an IL-33 inhibitor, offers a distinct mechanistic approach for patients, potentially addressing pathways not targeted by other available therapies. This novel mechanism may be a consideration for individuals who have not achieved optimal outcomes with agents acting on different inflammatory or bronchodilatory pathways. Specific efficacy data, dosing regimens, and indication breadth for Itepekimab are not provided in this context, suggesting its potential role may be further defined by its unique biological target.
In contrast, several established therapies provide defined efficacy profiles and diverse mechanisms. Dupilumab, an IL-4 receptor alpha antagonist, has shown a 30% reduction in the annualized rate of moderate or severe exacerbations at 52 weeks, with a dosing regimen of 300 mg subcutaneously every two weeks. Ensifentrine, a dual PDE3 and PDE4 inhibitor, demonstrated an 87mL change from baseline in FEV1 AUC0-12h at 12 weeks, administered as 3 mg twice daily via oral inhalation. Roflumilast, a PDE4 inhibitor, led to a 17% reduction in moderate or severe exacerbations at 52 weeks in COPD, dosed at 500 mcg orally once daily, and is also indicated for dermatologic conditions. Tiotropium, a long-acting muscarinic antagonist, offers once-daily dosing for COPD (18 mcg via dry powder inhaler or 5 mcg via inhalation spray) and asthma (2.5 mcg via inhalation spray). These alternatives may be selected based on their established efficacy, specific administration routes, or suitability for particular patient subgroups and comorbidities.
This information is for educational purposes only and does not constitute medical advice; clinical decisions regarding patient care belong with the prescribing clinician.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
itepekimabitepekimab alternativesalternativescomparisonchronic obstructive pulmonary diseaseil33-copditepekimab vs dupilumabitepekimab vs ensifentrineitepekimab vs roflumilastitepekimab vs tiotropiumitepekimab vs tozorakimab