Iptacopan is a complement factor B inhibitor approved for paroxysmal nocturnal hemoglobinuria, immunoglobulin A nephropathy, and complement 3 glomerulopathy. This page compares Iptacopan with Ravulizumab (Ultomiris), Pegcetacoplan (Empaveli, Syfovre), Crovalimab (PiaSky), Danicopan (Voydeya), and Pozelimab (Veopoz). Iptacopan's approved indications span multiple complement-mediated conditions, offering a broad therapeutic scope.
Iptacopan Alternatives: How It Compares to Other Complement Inhibitors
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 0/8 curated
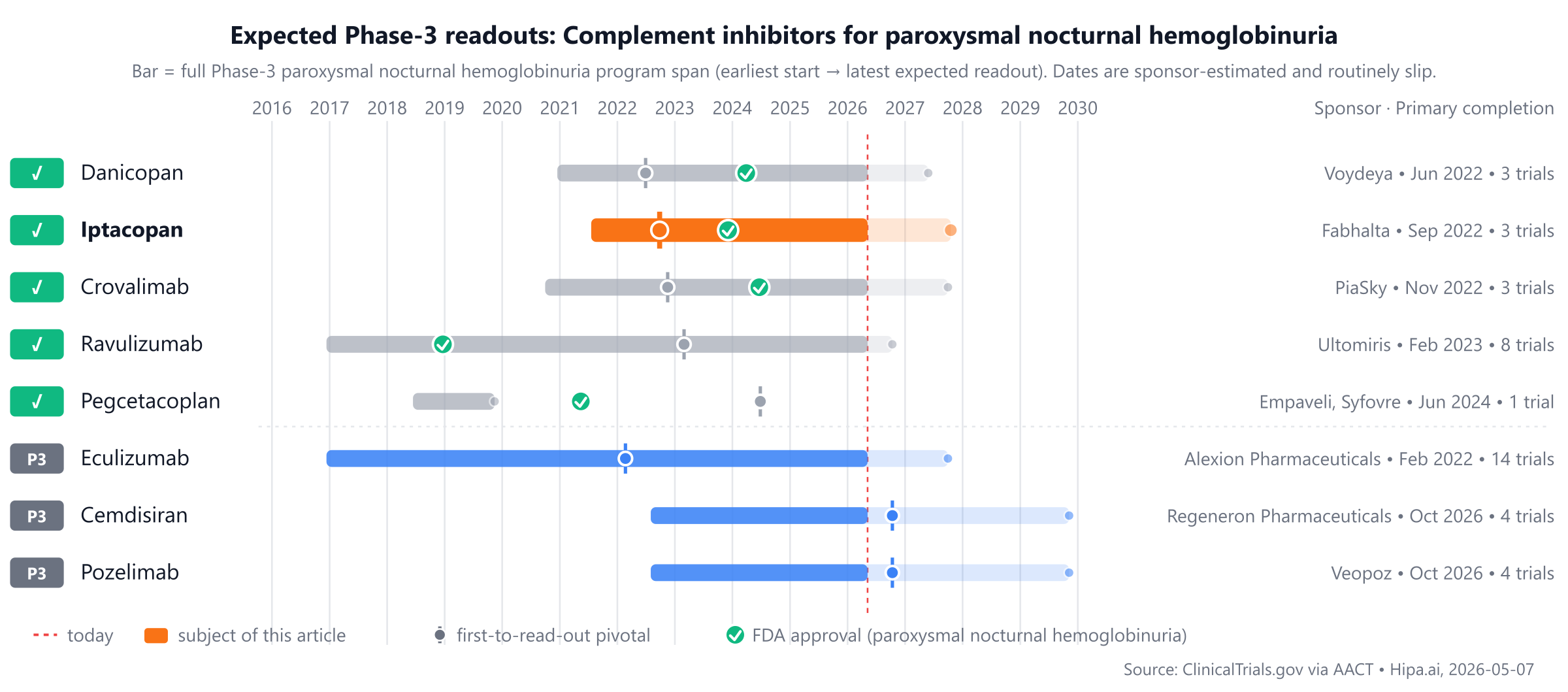
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape includes Ravulizumab (Ultomiris), approved in 2018, and Pegcetacoplan (Empaveli, Syfovre), approved in 2021. Iptacopan and Pozelimab (Veopoz) were approved in 2023, while other drugs like Eculizumab, Cemdisiran, and another Pozelimab formulation remain in Phase 3, trailing by approximately 1-2 years.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Iptacopan (Fabhalta) | Complement factor B inhibitor | paroxysmal nocturnal hemoglobinuria, immunoglobulin A nephropathy, complement 3 glomerulopathy | 200 mg orally twice daily | 2023 | Hemoglobin increase ≥ 2 g/dL without RBC transfusions: 82.3% @ 24 weeks | $550k |
| Ravulizumab (Ultomiris) | Complement C5 inhibitor | Paroxysmal nocturnal hemoglobinuria, Atypical hemolytic uremic syndrome, Generalized myasthenia gravis, +1 more | Weight-based intravenous loading dose on Day 1, followed by maintenance doses starting on Day 15 and every 8 weeks thereafter | 2018 | Transfusion avoidance: 73.6% @ 26 weeks | $520k |
| Pegcetacoplan (Empaveli, Syfovre) | Complement C3 inhibitor | Paroxysmal nocturnal hemoglobinuria (PNH), Geographic atrophy secondary to age-related macular degeneration, C3 glomerulopathy (C3G), +1 more | 1,080 mg twice weekly via subcutaneous infusion (Empaveli); intravitreal injection (Syfovre) | 2021 | Urine protein-to-creatinine ratio (UPCR) reduction: 68.3% @ 26 weeks | $517k |
| Danicopan (Voydeya) | Complement factor D inhibitor | Paroxysmal nocturnal hemoglobinuria | 150 mg orally three times daily | 2024 | Change in hemoglobin vs placebo: 2.44g/dL @ 12 weeks | $88k |
| Crovalimab (PiaSky) | Complement C5 inhibitor | Paroxysmal Nocturnal Hemoglobinuria | Weight-based tiered dosing. ≥40 kg to <100 kg: 1,000 mg IV on Day 1, then 340 mg SC weekly on Days 2, 8, 15, and 22; followed by 680 mg SC every 4 weeks starting Day 29. ≥100 kg: 1,500 mg IV on Day 1, then 340 mg SC weekly on Days 2, 8, 15, and 22; followed by 1,020 mg SC every 4 weeks starting Day 29. | 2024 | hemolysis control (LDH ≤1.5 × ULN): 79.3% @ week 5 to week 25 | — |
| Eculizumab | — | — | — | Pipeline | — | — |
| Cemdisiran | C5 inhibitor | — | Subcutaneous injection | Pipeline | — | — |
| Pozelimab (Veopoz) | Complement C5 inhibitor | CHAPLE disease | 30 mg/kg intravenous loading dose on Day 1, followed by 10 mg/kg subcutaneous injection once weekly starting on Day 8 | Pipeline | — | $1800k |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Hemoglobin improvement; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for paroxysmal nocturnal hemoglobinuria specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Iptacopan vs Ravulizumab (Ultomiris)
No head-to-head Phase-3 trial directly compares Iptacopan with Ravulizumab.
In separate pivotal trials, Iptacopan reported 82.3% Hemoglobin increase ≥ 2 g/dL without RBC transfusions at 24 weeks (NCT04558918) versus 73.6% Transfusion avoidance at 26 weeks for Ravulizumab (NCT02946463).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Iptacopan vs Pegcetacoplan (Empaveli, Syfovre)
No head-to-head Phase-3 trial directly compares Iptacopan with Pegcetacoplan.
In separate pivotal trials, Iptacopan reported 82.3% Hemoglobin increase ≥ 2 g/dL without RBC transfusions at 24 weeks (NCT04558918) versus 68.3% Urine protein-to-creatinine ratio (UPCR) reduction at 26 weeks for Pegcetacoplan (NCT05067127).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Iptacopan vs Crovalimab (PiaSky)
No head-to-head Phase-3 trial directly compares Iptacopan with Crovalimab.
In separate pivotal trials, Iptacopan reported 82.3% Hemoglobin increase ≥ 2 g/dL without RBC transfusions at 24 weeks (NCT04558918) versus 79.3% hemolysis control (LDH ≤1.5 × ULN) at week 5 to week 25 for Crovalimab (NCT04434092).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Iptacopan vs Danicopan (Voydeya)
No head-to-head Phase-3 trial directly compares Iptacopan with Danicopan.
In separate pivotal trials, Iptacopan reported 82.3% Hemoglobin increase ≥ 2 g/dL without RBC transfusions at 24 weeks (NCT04558918) versus 2.44g/dL Change in hemoglobin vs placebo at 12 weeks for Danicopan (NCT04469465).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Iptacopan vs Pozelimab (Veopoz)
No head-to-head Phase-3 trial directly compares Iptacopan with Pozelimab.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Several investigational drugs targeting the complement system are currently in active Phase 3 development. Eculizumab, from Alexion Pharmaceuticals, Inc., is being evaluated in a lead Phase 3 trial, NCT03056040. Also in Phase 3, Cemdisiran and Pozelimab, both developed by Regeneron Pharmaceuticals, are being investigated in a shared lead trial, NCT05133531. These agents primarily target C5, representing a different mechanism of complement inhibition compared to Factor B inhibitors like Iptacopan.
Choosing between Iptacopan and its alternatives
Iptacopan, as a complement factor B inhibitor, presents a distinct mechanism of action within the complement cascade compared to agents targeting C3 or C5. A key differentiator for iptacopan is its oral administration, which may offer convenience for patients when compared to therapies requiring intravenous or subcutaneous infusions. While specific efficacy data for iptacopan are not provided here, its unique target within the complement system may be a consideration for clinicians seeking alternative approaches to complement inhibition.
Conversely, other complement inhibitors offer established profiles and varied administration schedules. Ravulizumab, a C5 inhibitor, demonstrated transfusion avoidance in 73.6% of patients at 26 weeks with an every 8-week intravenous dosing schedule. Crovalimab, another C5 inhibitor, achieved hemolysis control (LDH ≤1.5 × ULN) in 79.3% of patients from week 5 to week 25, with a tiered weight-based dosing regimen that includes weekly subcutaneous injections after an initial intravenous dose. Pegcetacoplan, a C3 inhibitor, showed a 68.3% reduction in urine protein-to-creatinine ratio at 26 weeks, administered twice weekly via subcutaneous infusion (Empaveli). Danicopan, a factor D inhibitor, led to a 2.44g/dL change in hemoglobin versus placebo at 12 weeks with oral dosing three times daily. These agents present different mechanisms, efficacy profiles, and dosing frequencies, which clinicians may consider based on individual patient needs, disease characteristics, and established experience with specific therapies.
This information is for educational purposes only and does not constitute medical advice; clinical decisions should always be made by a qualified prescriber in consultation with their patient.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
iptacopaniptacopan alternativesalternativescomparisonparoxysmal nocturnal hemoglobinuriafactor-b-pnhiptacopan vs eculizumabiptacopan vs ravulizumabiptacopan vs pegcetacoplaniptacopan vs crovalimabiptacopan vs danicopan