Frexalimab is an investigational CD40L inhibitor, a class of drugs designed to modulate immune responses. This page compares Frexalimab to other treatments such as Ocrelizumab (Ocrevus), Ofatumumab (Kesimpta), Teriflunomide (Aubagio), and Fingolimod (Gilenya). Its distinct mechanism of action targets a different pathway compared to many established therapies.
Frexalimab Alternatives: How It Compares to Other Multiple Sclerosis Therapies
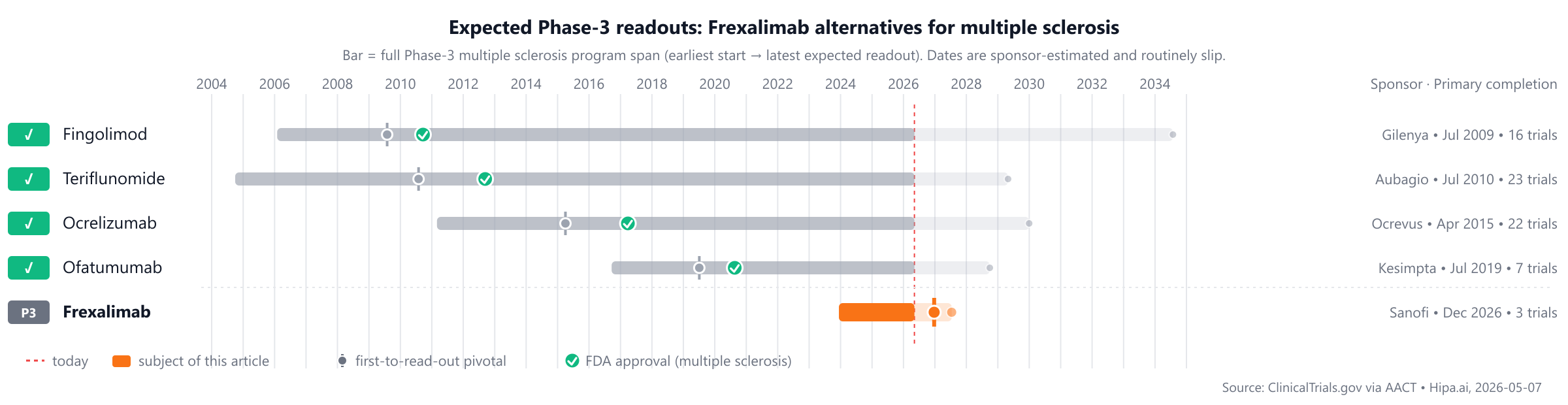
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: AI-augmented data · 0/5 curated
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape features established comparators such as Ofatumumab (Kesimpta), approved in 2009, and Fingolimod (Gilenya), approved in 2010, with Frexalimab currently not yet approved.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Frexalimab | CD40L inhibitor | — | Intravenous (IV) infusion or subcutaneous (SC) injection | Pipeline | — | — |
| Fingolimod (Gilenya) | Sphingosine 1-phosphate (S1P) receptor modulator | multiple sclerosis | 0.5 mg orally once daily | 2010 | 0.18relapses/year @ 24 months | $96k |
| Teriflunomide (Aubagio) | Pyrimidine synthesis inhibitor | Multiple sclerosis | 7 mg or 14 mg orally once daily | 2012 | 31.5% @ 108 weeks | $110k |
| Ocrelizumab (Ocrevus) | Anti-CD20 monoclonal antibody | Multiple Sclerosis | Initial dose of 300 mg IV infusion, followed 2 weeks later by a second 300 mg IV infusion. Maintenance dose of 600 mg IV infusion every 6 months. | 2017 | 0.16relapses/year @ 96 weeks | $70k |
| Ofatumumab (Kesimpta) | Anti-CD20 monoclonal antibody | Chronic Lymphocytic Leukemia, Multiple Sclerosis | 20 mg subcutaneously once monthly (following initial loading doses at weeks 0, 1, and 2) | 2020 | 0.11relapses/year @ up to 30 months | $118k |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Annualized Relapse Rate (ARR); cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for multiple sclerosis specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Frexalimab vs Ocrelizumab (Ocrevus)
No head-to-head Phase-3 trial directly compares Frexalimab with Ocrelizumab.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Frexalimab vs Ofatumumab (Kesimpta)
No head-to-head Phase-3 trial directly compares Frexalimab with Ofatumumab.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Frexalimab vs Teriflunomide (Aubagio)
The pivotal head-to-head evidence comes from a head-to-head Phase-3 trial (NCT06141473) enrolling 1,600 participants, primary completion 2027-05.
Primary-endpoint values for NCT06141473 are not yet posted in the AACT results database.
Source: ClinicalTrials.gov via AACT — pulled directly from the trial's posted results. View the full trial record.
Frexalimab vs Fingolimod (Gilenya)
No head-to-head Phase-3 trial directly compares Frexalimab with Fingolimod.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Choosing between Frexalimab and its alternatives
Frexalimab, a CD40L inhibitor, represents a novel mechanistic approach to multiple sclerosis management, distinct from established B-cell depleters or oral therapies. Its unique target may offer an alternative for patients who have not responded adequately to other treatment pathways or for whom a different immunomodulatory strategy is desired. While specific efficacy and dosing data for Frexalimab are still emerging, its mechanism introduces a new option in the therapeutic landscape.
In contrast, several well-established therapies offer diverse profiles with extensive clinical experience. Ocrelizumab (Ocrevus), an anti-CD20 monoclonal antibody, has demonstrated an annualized relapse rate (ARR) of 0.16 relapses per year over 96 weeks with its twice-yearly intravenous dosing. Another anti-CD20 option, Ofatumumab (Kesimpta), offers monthly subcutaneous administration and has shown an ARR of 0.11 relapses per year over up to 30 months. For patients preferring oral daily regimens, Teriflunomide (Aubagio), a pyrimidine synthesis inhibitor, reduced ARR by 31.5% over 108 weeks, while Fingolimod (Gilenya), an S1P receptor modulator, reported an ARR of 0.18 relapses per year at 24 months. These agents, with their longer clinical track records and varied mechanisms, may be considered based on factors such as administration preference, specific safety profiles, and patient comorbidities.
This information is for educational purposes only and is not medical advice; clinical decisions belong with the prescriber.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Head-to-head trials cited on this page:
- NCT06141473: Frexalimab vs Teriflunomide · Efficacy and Safety Studies of Frexalimab (SAR441344) in Adults With Relapsing Forms of Multiple Sclerosis
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
frexalimabfrexalimab alternativesalternativescomparisonmultiple sclerosiscd40l-multiple-sclerosisfrexalimab vs ocrelizumabfrexalimab vs ofatumumabfrexalimab vs teriflunomidefrexalimab vs fingolimod