EYP-1901 is a Tyrosine kinase inhibitor. This page compares EYP-1901 with established anti-VEGF agents such as Aflibercept (Eylea), Ranibizumab (Lucentis), Brolucizumab (Beovu), Faricimab (Vabysmo), and Bevacizumab (Avastin). Its distinct mechanism of action as a Tyrosine kinase inhibitor may offer different therapeutic considerations compared to these anti-VEGF biologics.
EYP-1901 Alternatives: How It Compares to Other Anti-VEGF Therapies
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: AI-augmented data · 0/8 curated
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
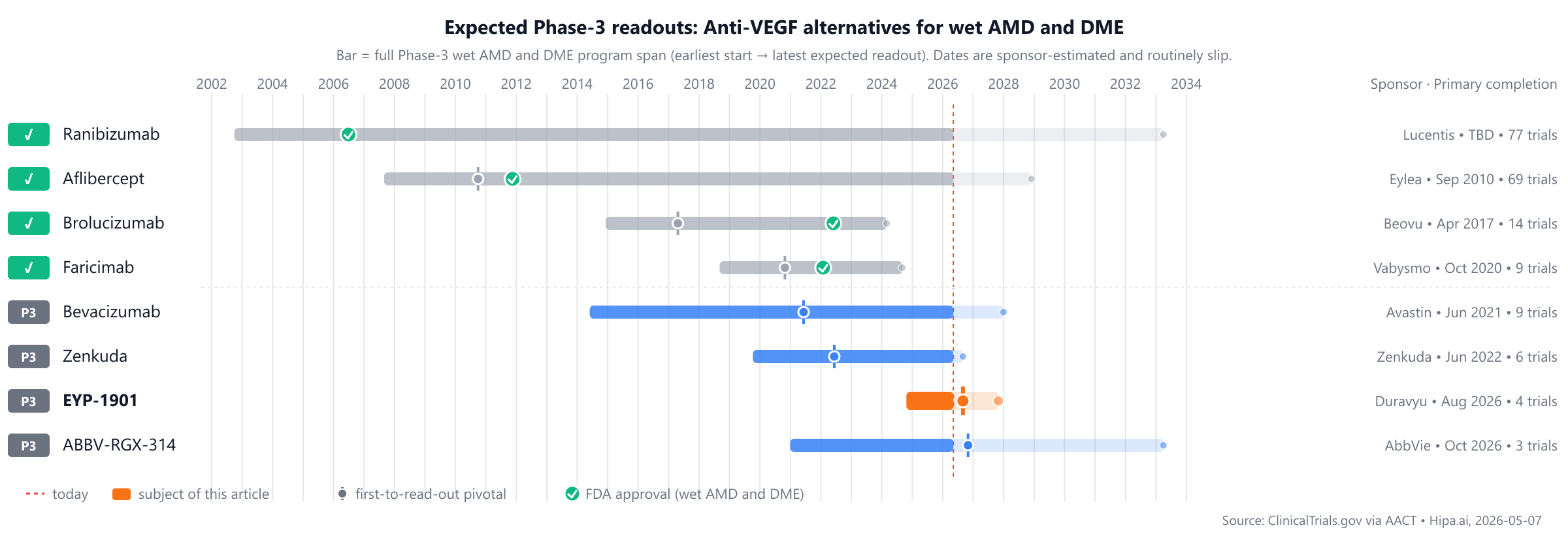
The market is dominated by long-approved treatments such as Avastin (approved 2004) and Lucentis (approved 2006), with EYP-1901 positioned as a newer entrant yet to be approved. Several pipeline drugs, including Zenkuda and ABBV-RGX-314, are also in Phase 3, appearing approximately 1-2 years behind EYP-1901's current stage.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| EYP-1901 (Duravyu) | Tyrosine kinase inhibitor | — | Intravitreal insert every 6 months | Pipeline | — | — |
| Ranibizumab (Lucentis) | VEGF inhibitor | wet AMD, macular edema following retinal vein occlusion, diabetic macular edema, +2 more | 0.5 mg by intravitreal injection once a month (approximately 28 days) | 2006 | Proportion of patients losing <15 letters: 94.6% @ 12 months | $23k |
| Aflibercept (Eylea) | VEGF inhibitor | Wet age-related macular degeneration, Macular edema following retinal vein occlusion, Diabetic macular edema, +2 more | 2 mg administered by intravitreal injection every 4 weeks for the first 3 months, followed by 2 mg every 8 weeks | 2011 | proportion of patients maintaining visual acuity (<15 letters lost): 95.1% @ 52 weeks | $12k |
| Faricimab (Vabysmo) | Bispecific VEGF-A/Ang-2 inhibitor | wet AMD, diabetic macular edema, macular edema following retinal vein occlusion | 6 mg administered by intravitreal injection every 4 weeks for the first 4 doses, followed by individualized dosing intervals up to every 16 weeks. | 2022 | Change from baseline in Best-Corrected Visual Acuity (BCVA): 5.8letters @ 48 weeks | $15k |
| Brolucizumab (Beovu) | VEGF inhibitor | wet age-related macular degeneration, diabetic macular edema | 6 mg by intravitreal injection. For wet AMD: monthly for the first 3 doses, then every 8-12 weeks. For DME: every 6 weeks for the first 5 doses, then every 8-12 weeks. | 2022 | 6.6ETDRS letters @ week 48 | $7k |
| Bevacizumab (Avastin) | VEGF inhibitor | Colorectal cancer, Non-small cell lung cancer, Glioblastoma, +6 more | 5 mg/kg to 15 mg/kg intravenous infusion every 2 to 3 weeks | Pipeline | — | — |
| Zenkuda (Zenkuda) | VEGF inhibitor | — | — | Pipeline | — | — |
| ABBV-RGX-314 | Anti-VEGF AAV8 gene therapy | — | One-time subretinal or suprachoroidal injection | Pipeline | — | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Change in BCVA; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for wet AMD and DME specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
EYP-1901 vs Aflibercept (Eylea)
The pivotal head-to-head evidence comes from a head-to-head Phase-3 trial (NCT06683742) enrolling 400 participants, primary completion 2026-10.
Primary-endpoint values for NCT06683742 are not yet posted in the AACT results database.
Source: ClinicalTrials.gov via AACT — pulled directly from the trial's posted results. View the full trial record.
EYP-1901 vs Ranibizumab (Lucentis)
No head-to-head Phase-3 trial directly compares EYP-1901 with Ranibizumab.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
EYP-1901 vs Brolucizumab (Beovu)
No head-to-head Phase-3 trial directly compares EYP-1901 with Brolucizumab.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
EYP-1901 vs Faricimab (Vabysmo)
No head-to-head Phase-3 trial directly compares EYP-1901 with Faricimab.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
EYP-1901 vs Bevacizumab (Avastin)
No head-to-head Phase-3 trial directly compares EYP-1901 with Bevacizumab.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Several investigational drugs are currently in active Phase 3 development. These include **Bevacizumab** from Outlook Therapeutics, Inc., being evaluated in a lead Phase 3 trial NCT03834753. Kodiak Sciences Inc. is developing **Zenkuda**, with its lead Phase 3 trial identified as NCT04592419. Additionally, AbbVie is advancing **ABBV-RGX-314**, which is undergoing investigation in a lead Phase 3 trial NCT05407636.
Choosing between EYP-1901 and its alternatives
EYP-1901, a tyrosine kinase inhibitor, offers a distinct mechanism of action compared to direct vascular endothelial growth factor (VEGF) inhibitors. This difference may be a primary consideration when selecting a therapy, particularly for patients where a novel mechanistic approach is desired or when response to existing anti-VEGF agents is suboptimal. The unique pathway targeted by EYP-1901 could present an alternative strategy in managing retinal conditions.
Conversely, other anti-VEGF therapies offer established efficacy, diverse dosing schedules, and varying mechanisms. For instance, aflibercept has demonstrated a high proportion of patients maintaining visual acuity (95.1% at 52 weeks) with dosing every 8 weeks after initial loading. Similarly, ranibizumab has shown 94.6% of patients losing less than 15 letters at 12 months, typically with monthly administration. For patients seeking less frequent injections, faricimab, a bispecific VEGF-A/Ang-2 inhibitor, can be individualized up to every 16 weeks following initial doses, and brolucizumab offers dosing every 8-12 weeks after loading. Bevacizumab may be considered in situations where cost-effectiveness is a significant factor. The choice among these agents often balances factors such as established clinical experience, desired injection frequency, and specific mechanistic considerations.
This information is for educational purposes and does not constitute medical advice; clinical decisions regarding patient care should always be made by a qualified healthcare prescriber.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Head-to-head trials cited on this page:
- NCT06683742: EYP-1901 vs Aflibercept · A 2-year Study of EYP-1901 in Subjects With Wet Age Related Macular Degeneration (wAMD) (LUCIA) Primary Efficacy Will be…
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
eyp-1901eyp-1901 alternativesalternativescomparisonwet AMD and DMEanti-vegf-wamd-dmeeyp-1901 vs aflibercepteyp-1901 vs ranibizumabeyp-1901 vs brolucizumabeyp-1901 vs faricimabeyp-1901 vs bevacizumab