Etavopivat is a pyruvate kinase R (PKR) activator. This page compares Etavopivat with other treatments, including Mitapivat (Pyrukynd, Aqvesme), Crizanlizumab (Adakveo), L-glutamine (Endari), Casgevy, and LentiGlobin BB305 (Lyfgenia, Zynteglo), highlighting their distinct mechanisms and administration routes.
Etavopivat Alternatives: How It Compares to Other Sickle Cell Disease Therapies
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: AI-augmented data · 0/8 curated
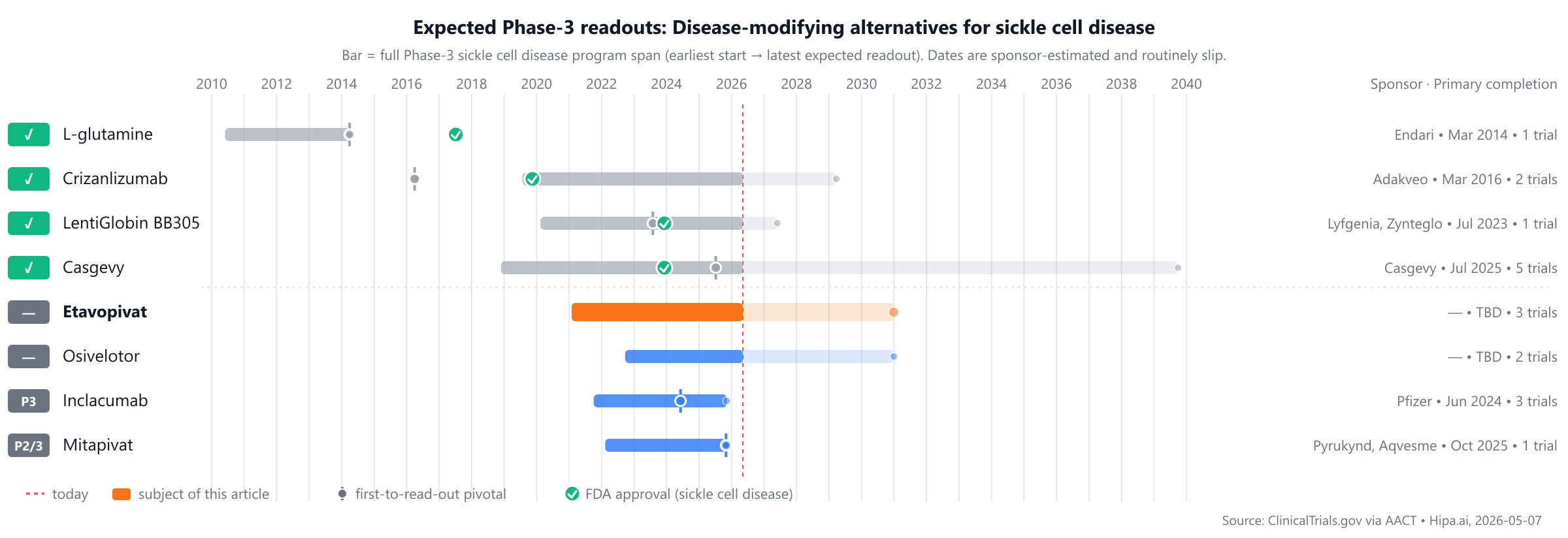
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape includes approved therapies such as L-glutamine (Endari, 2004) and Crizanlizumab (Adakveo, 2019), while Etavopivat is not yet approved. Several pipeline drugs, including Mitapivat, Inclacumab, and Osivelotor, are currently in Phase 3 and appear to be approximately 1-2 years behind.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Etavopivat | PKR activator | — | 400 mg orally once daily | Pipeline | Hemoglobin response (>1 g/dL increase): 48.7% @ 24 weeks | — |
| L-glutamine (Endari) | Amino acid | short bowel syndrome, sickle cell disease | 5 to 15 g orally twice daily, based on body weight | 2017 | median sickle cell crises: 3crises @ 48 weeks | $42k |
| Crizanlizumab (Adakveo) | P-selectin inhibitor | sickle cell disease | 5 mg/kg administered by intravenous infusion at week 0, week 2, and every 4 weeks thereafter | 2019 | reduction in median annual rate of vaso-occlusive crises: 45.3% @ 52 weeks | $132k |
| Casgevy (Casgevy) | CRISPR/Cas9 gene-edited cell therapy | sickle cell disease, transfusion-dependent beta thalassemia | Single intravenous infusion | 2023 | freedom from severe vaso-occlusive crises for at least 12 consecutive months: 93.5% @ 24 months | $2200k |
| LentiGlobin BB305 (Lyfgenia, Zynteglo) | Cell-based gene therapy | beta-thalassemia, sickle cell disease | Single-dose intravenous infusion | 2023 | Complete resolution of vaso-occlusive events (VOE-CR): 88% @ 6 to 18 months | $3100k |
| Mitapivat (Pyrukynd, Aqvesme) | Pyruvate kinase activator | Pyruvate kinase deficiency, Alpha- or beta-thalassemia | 5 mg, 20 mg, or 50 mg orally twice daily | Pipeline | Hemoglobin response: 42.3% @ 24 weeks | $335k |
| Inclacumab | P-selectin inhibitor | — | 30 mg/kg intravenously every 12 weeks | Pipeline | — | — |
| Osivelotor | Hemoglobin S polymerization inhibitor | — | — | Pipeline | Change from baseline in hemoglobin: 3.17g/dL @ 12 weeks | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Annualized VOC rate; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for sickle cell disease specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Etavopivat vs Mitapivat (Pyrukynd, Aqvesme)
No head-to-head Phase-3 trial directly compares Etavopivat with Mitapivat.
In separate pivotal trials, Etavopivat reported 48.7% Hemoglobin response (>1 g/dL increase) at 24 weeks (NCT04624659) versus 42.3% Hemoglobin response at 24 weeks for Mitapivat (NCT04770753).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Etavopivat vs Crizanlizumab (Adakveo)
No head-to-head Phase-3 trial directly compares Etavopivat with Crizanlizumab.
In separate pivotal trials, Etavopivat reported 48.7% Hemoglobin response (>1 g/dL increase) at 24 weeks (NCT04624659) versus 45.3% reduction in median annual rate of vaso-occlusive crises at 52 weeks for Crizanlizumab (NCT01895361).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Etavopivat vs L-glutamine (Endari)
No head-to-head Phase-3 trial directly compares Etavopivat with L-glutamine.
In separate pivotal trials, Etavopivat reported 48.7% Hemoglobin response (>1 g/dL increase) at 24 weeks (NCT04624659) versus 3crises median sickle cell crises at 48 weeks for L-glutamine (NCT01179217).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Etavopivat vs Casgevy (Casgevy)
No head-to-head Phase-3 trial directly compares Etavopivat with Casgevy.
In separate pivotal trials, Etavopivat reported 48.7% Hemoglobin response (>1 g/dL increase) at 24 weeks (NCT04624659) versus 93.5% freedom from severe vaso-occlusive crises for at least 12 consecutive months at 24 months for Casgevy (NCT03745287).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Etavopivat vs LentiGlobin BB305 (Lyfgenia, Zynteglo)
No head-to-head Phase-3 trial directly compares Etavopivat with LentiGlobin BB305.
In separate pivotal trials, Etavopivat reported 48.7% Hemoglobin response (>1 g/dL increase) at 24 weeks (NCT04624659) versus 88% Complete resolution of vaso-occlusive events (VOE-CR) at 6 to 18 months for LentiGlobin BB305 (NCT02140554).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Several investigational IL-17 / IL-17-related drugs are currently in active Phase 3 development. Among these is Mitapivat, sponsored by Agios Pharmaceuticals, Inc., with its lead Phase 3 trial registered as NCT05031780. Also in Phase 3 is Inclacumab from Pfizer, with its primary Phase 3 study identified as NCT04935879. Another investigational agent in this category is Osivelotor, for which the sponsor is currently unknown.
Choosing between Etavopivat and its alternatives
Etavopivat, a pyruvate kinase (PKR) activator, offers a targeted approach to managing sickle cell disease by modulating red blood cell metabolism. For patients seeking an oral therapy, Etavopivat may be considered, potentially offering a convenient dosing regimen. Its mechanism of action distinguishes it from P-selectin inhibitors or amino acid supplements, which may appeal to individuals who have not responded adequately to other approaches or are seeking a different therapeutic pathway.
Alternative therapies present varied profiles that may be preferred depending on patient-specific factors. Mitapivat (Pyrukynd, Aqvesme), also a pyruvate kinase activator, demonstrated a 42.3% hemoglobin response at 24 weeks with its oral dosing options. For patients primarily experiencing vaso-occlusive crises, Crizanlizumab (Adakveo), a P-selectin inhibitor, reduced the median annual rate of crises by 45.3% over 52 weeks via intravenous infusion. L-glutamine (Endari), an amino acid, showed a median of 3 sickle cell crises over 48 weeks and may be considered for its different mechanism and oral administration. For those with severe disease or who have exhausted other options, gene therapies like Casgevy and Lyfgenia (Zynteglo) offer substantial efficacy. Casgevy achieved freedom from severe vaso-occlusive crises for at least 12 consecutive months in 93.5% of patients at 24 months, while Lyfgenia demonstrated 88% complete resolution of vaso-occlusive events. These gene therapies involve a single intravenous infusion but represent a more intensive intervention.
Clinical decisions regarding specific therapies should always be made by the prescribing clinician in consultation with the patient.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
etavopivatetavopivat alternativesalternativescomparisonsickle cell diseasedisease-modifying-sickle-celletavopivat vs mitapivatetavopivat vs crizanlizumabetavopivat vs l-glutamineetavopivat vs casgevyetavopivat vs lentiglobin bb305