Elranatamab is a BCMA-directed CD3 bispecific antibody approved for the treatment of multiple myeloma. This page compares Elranatamab to other therapies targeting BCMA, including Teclistamab (Tecvayli), Linvoseltamab (Lynozyfic), Cilta-cel (Carvykti), and Idecabtagene vicleucel (Abecma). These therapies offer varied approaches to BCMA targeting, including differences in administration routes and treatment schedules.
Elranatamab Alternatives: How It Compares to Other BCMA-Directed Therapies
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 0/8 curated
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
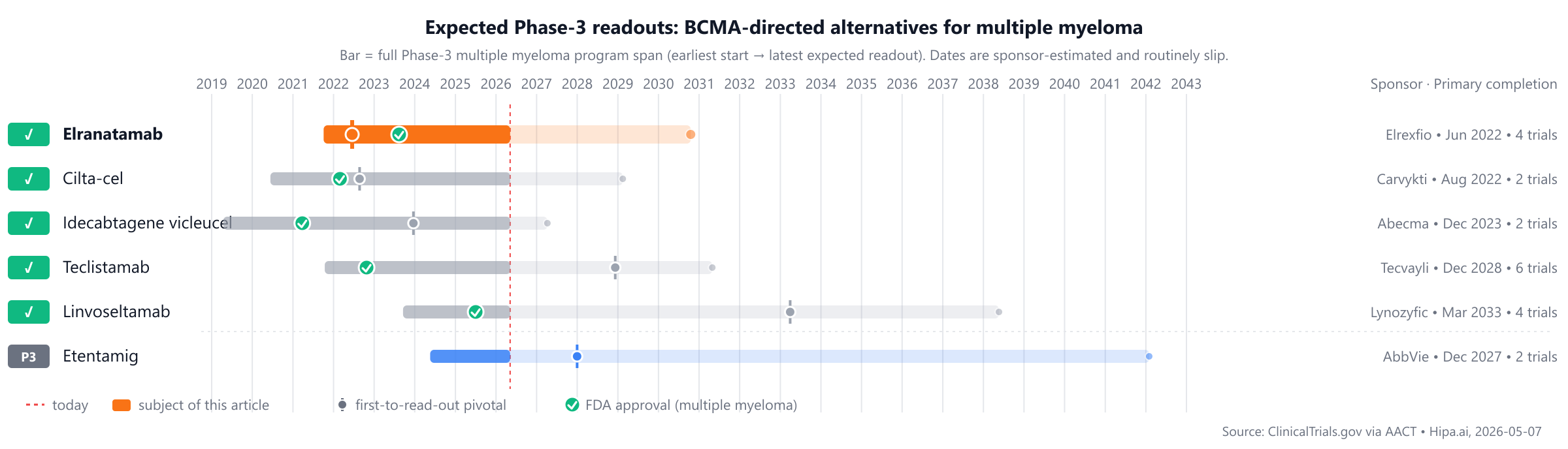
The competitive landscape includes approved therapies such as Abecma (approved 2021) and Carvykti (approved 2022), with Elranatamab joining the market in 2023. Several pipeline drugs, including Belantamab-mafodotin, Etentamig, and Anitocabtagene autoleucel, remain in Phase 3, positioning them approximately 1-2 years behind the most recent market approvals.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Elranatamab (Elrexfio) | BCMA-directed CD3 bispecific antibody | Multiple myeloma | Step-up doses of 12 mg on Day 1 and 32 mg on Day 4, followed by 76 mg subcutaneously once weekly starting on Day 8 through Week 24. After 24 weeks, responders may transition to 76 mg every 2 weeks, and subsequently every 4 weeks if response is maintained. | 2023 | 57.7% @ 11.1 months median follow-up | $330k |
| Idecabtagene vicleucel (Abecma) | BCMA-directed CAR T-cell therapy | multiple myeloma | Single-dose intravenous infusion | 2021 | 72% @ best overall response | $420k |
| Cilta-cel (Carvykti) | BCMA-directed CAR-T cell therapy | multiple myeloma | Single intravenous infusion of 0.5-1.0 x 10^6 CAR-positive viable T cells/kg (maximum 1 x 10^8 cells) | 2022 | 97.9% @ 18 months | $465k |
| Teclistamab (Tecvayli) | BCMA-directed CD3 bispecific T-cell engager | relapsed or refractory multiple myeloma | Step-up doses of 0.06 mg/kg and 0.3 mg/kg, followed by 1.5 mg/kg subcutaneously once weekly until disease progression or unacceptable toxicity (may be reduced to biweekly or monthly in responding patients) | 2022 | 89% @ 34.5 months | $474k |
| Linvoseltamab (Lynozyfic) | BCMAxCD3 bispecific antibody | Relapsed or refractory multiple myeloma | Intravenous infusion: 5 mg on day 1, 25 mg on day 8, 200 mg on day 15; then 200 mg weekly (weeks 4-13), every 2 weeks (weeks 14-24), and every 4 weeks thereafter (if VGPR or better is achieved). | 2025 | 70% @ median 13 months | $454k |
| Belantamab-mafodotin | — | — | — | Pipeline | — | — |
| Etentamig | BCMA-directed bispecific T-cell engager | — | 60 mg intravenously every 4 weeks | Pipeline | — | — |
| Anitocabtagene autoleucel | BCMA-directed CAR-T cell therapy | — | Single intravenous infusion | Pipeline | 97% @ Best overall response | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is ORR; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for multiple myeloma specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Elranatamab vs Teclistamab (Tecvayli)
No head-to-head Phase-3 trial directly compares Elranatamab with Teclistamab.
In separate pivotal trials, Elranatamab reported 57.7% ORR at 11.1 months median follow-up (NCT04649359) versus 89% ORR at 34.5 months for Teclistamab (NCT05083169).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Elranatamab vs Linvoseltamab (Lynozyfic)
No head-to-head Phase-3 trial directly compares Elranatamab with Linvoseltamab.
In separate pivotal trials, Elranatamab reported 57.7% ORR at 11.1 months median follow-up (NCT04649359) versus 70% ORR at median 13 months for Linvoseltamab (NCT03761108).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Elranatamab vs Cilta-cel (Carvykti)
No head-to-head Phase-3 trial directly compares Elranatamab with Cilta-cel.
In separate pivotal trials, Elranatamab reported 57.7% ORR at 11.1 months median follow-up (NCT04649359) versus 97.9% ORR at 18 months for Cilta-cel (NCT03548207).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Elranatamab vs Idecabtagene vicleucel (Abecma)
No head-to-head Phase-3 trial directly compares Elranatamab with Idecabtagene vicleucel.
In separate pivotal trials, Elranatamab reported 57.7% ORR at 11.1 months median follow-up (NCT04649359) versus 72% ORR at best overall response for Idecabtagene vicleucel (NCT03361748).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Among investigational agents in active Phase-3 development, Etentamig from AbbVie is an IL-17A nanobody, with its lead Phase-3 trial identified as NCT06158841. This agent represents a different mechanism compared to Elranatamab, specifically targeting IL-17A. Other investigational agents in active Phase-3 development include Belantamab-mafodotin and Anitocabtagene autoleucel, though sponsors for these agents are not specified in the provided data.
Choosing between Elranatamab and its alternatives
Elranatamab, a BCMA-directed CD3 bispecific antibody, offers a potential treatment option for patients with multiple myeloma. As a bispecific T-cell engager, it shares a mechanism of action with agents like Teclistamab and Linvoseltamab, facilitating T-cell redirection to BCMA-expressing myeloma cells. Its subcutaneous administration route may offer flexibility in care settings compared to intravenous options or the complex logistics associated with CAR T-cell therapies such as Cilta-cel or Idecabtagene vicleucel. While specific efficacy data for Elranatamab is not detailed here, its place within the bispecific class suggests it may be considered for patients seeking an off-the-shelf option with a convenient dosing schedule.
For some patients, alternative BCMA-directed therapies may be preferred based on established efficacy profiles and administration considerations. Teclistamab, another BCMA-directed CD3 bispecific T-cell engager, has demonstrated an overall response rate of 89% with a median follow-up of 34.5 months, providing a longer track record of observed outcomes. Linvoseltamab, also a BCMAxCD3 bispecific antibody, showed an ORR of 70% at a median of 13 months. In cases where a single-infusion cellular therapy is considered, BCMA-directed CAR T-cell therapies like Cilta-cel (overall response rate 97.9% at 18 months) or Idecabtagene vicleucel (ORR 72%) may be chosen, despite requiring a manufacturing lead time. These CAR T-cell options offer a distinct mechanism that could be considered for specific patient subgroups.
This information is not medical advice; clinical decisions should always be made by the prescribing clinician in consultation with their patient.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
elranatamabelranatamab alternativesalternativescomparisonmultiple myelomabcma-bispecific-multiple-myelomaelranatamab vs teclistamabelranatamab vs linvoseltamabelranatamab vs cilta-celelranatamab vs idecabtagene vicleucelelranatamab vs belantamab-mafodotin