Divarasib is a KRAS G12C inhibitor. This page provides a comparison of Divarasib with other agents in its class.
Divarasib Alternatives: How It Compares to Other KRAS G12C Inhibitors
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 0/3 curated
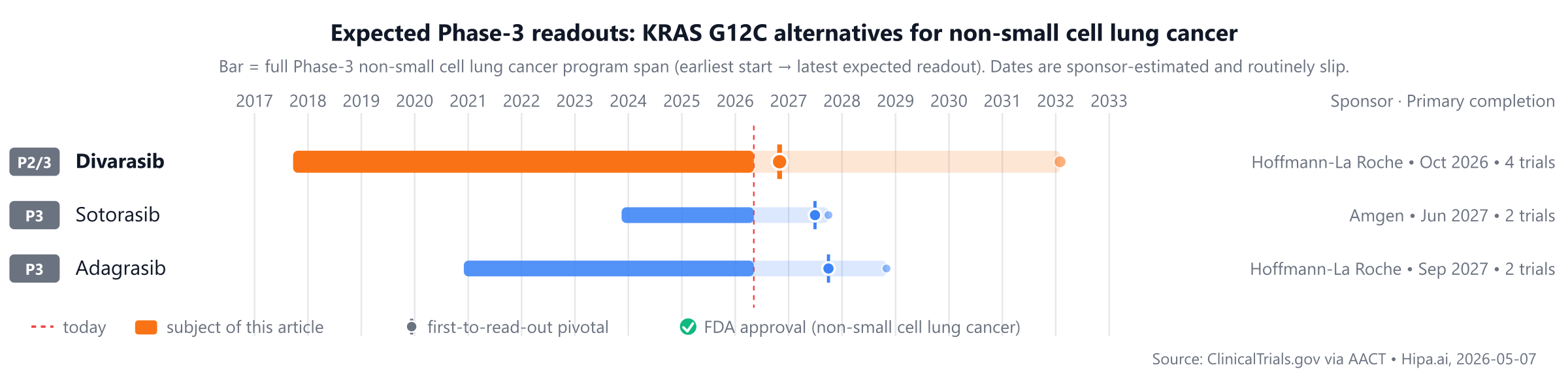
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
Divarasib is an approved comparator, while Sotorasib and Adagrasib are currently in Phase 3 development, approximately 1-2 years behind.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Divarasib | KRAS G12C inhibitor | — | 400 mg orally once daily | Pipeline | — | — |
| Sotorasib | — | — | — | Pipeline | — | — |
| Adagrasib | — | — | — | Pipeline | — | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Objective Response Rate (ORR); cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for non-small cell lung cancer specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Pipeline alternatives
Several investigational IL-17 / IL-17-related drugs are currently in active Phase 3 development. Sotorasib, sponsored by Amgen, is being evaluated in a lead Phase 3 trial, NCT05920356. Another agent, Adagrasib, developed by Hoffmann-La Roche, is also in Phase 3, with its lead trial identified as NCT06497556.
Choosing between Divarasib and its alternatives
When selecting a KRAS G12C inhibitor, clinicians weigh various factors. Divarasib may be considered when its specific profile aligns with patient needs. If clinical data indicate a differentiated efficacy magnitude in particular patient populations or disease settings, this could influence its selection. Furthermore, potential advantages in dosing convenience or a broader indication profile, should these be established through clinical trials, would be key considerations favoring Divarasib.
Conversely, alternative KRAS G12C inhibitors might be preferred in situations where a longer track record of clinical use and real-world experience is a primary concern. Differences in cost-effectiveness or a distinct safety profile, if demonstrated in comparative studies, could also guide treatment decisions. For specific patient subgroups, an alternative agent might offer a unique mechanism or therapeutic advantage that is particularly relevant to their clinical presentation or comorbidities.
This information is not medical advice; clinical decisions belong with the prescriber.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Head-to-head trials cited on this page:
- NCT06497556: Divarasib vs Sotorasib · A Study Evaluating the Efficacy and Safety of Divarasib Versus Sotorasib or Adagrasib in Participants With Previously Tr…
- NCT06497556: Divarasib vs Adagrasib · A Study Evaluating the Efficacy and Safety of Divarasib Versus Sotorasib or Adagrasib in Participants With Previously Tr…
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
divarasibdivarasib alternativesalternativescomparisonnon-small cell lung cancerkras-g12c-nsclcdivarasib vs sotorasibdivarasib vs adagrasib