Depemokimab is an interleukin-5 (IL-5) inhibitor approved for the treatment of severe asthma. This page compares Depemokimab to other IL-5 inhibitors, including Mepolizumab (Nucala), Benralizumab (Fasenra), and Reslizumab (Cinqair). While all target the IL-5 pathway, differences in their mechanisms of action or dosing schedules may influence treatment selection.
Depemokimab Alternatives: How It Compares to Other IL-5 Inhibitors
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: AI-augmented data · 0/4 curated
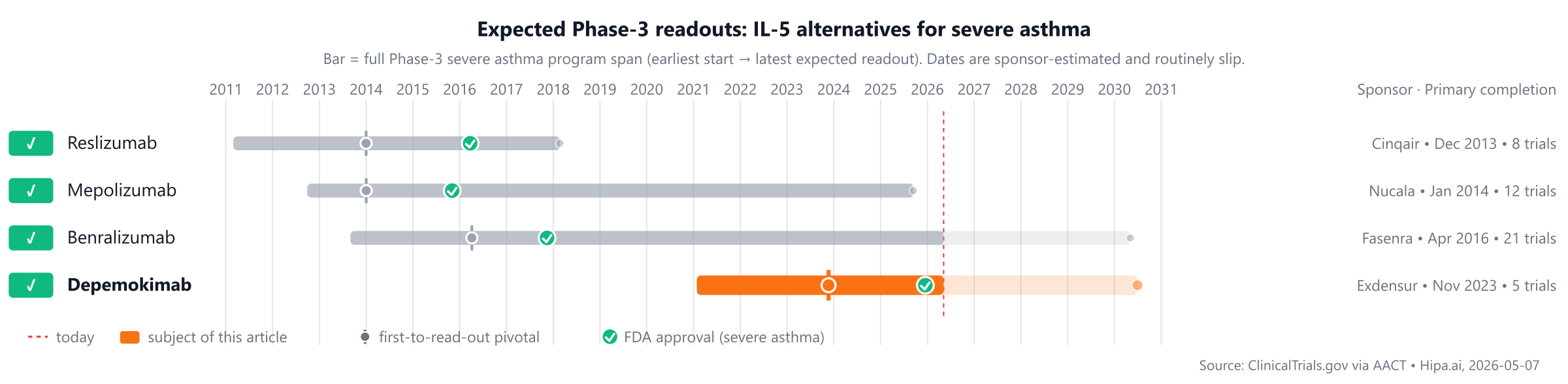
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
The competitive landscape for this indication includes long-established treatments such as Mepolizumab (Nucala) approved in 2015 and Reslizumab (Cinqair) in 2016, with Depemokimab entering the market much later in 2025 and no other Phase 3 pipeline drugs currently identified.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Depemokimab (Exdensur) | IL-5 inhibitor | Severe asthma | 100 mg subcutaneously every 6 months | 2025 | 58% @ 52 weeks | — |
| Mepolizumab (Nucala) | IL-5 inhibitor | severe asthma, eosinophilic granulomatosis with polyangiitis, hypereosinophilic syndrome, +2 more | 100 mg subcutaneously once every 4 weeks | 2015 | 53% @ 32 weeks | $47k |
| Reslizumab (Cinqair) | IL-5 inhibitor | Severe asthma | 3 mg/kg IV infusion once every 4 weeks | 2016 | Reduction in clinical asthma exacerbations: 50% @ 52 weeks | $32k |
| Benralizumab (Fasenra) | IL-5 receptor antagonist | Severe asthma, Eosinophilic granulomatosis with polyangiitis | 30 mg subcutaneously every 4 weeks for the first 3 doses, then once every 8 weeks | 2017 | Annual asthma exacerbation rate (AER) reduction: 51% @ 48 weeks | $38k |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Annualized asthma exacerbation rate; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for severe asthma specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Depemokimab vs Mepolizumab (Nucala)
The pivotal head-to-head evidence comes from a head-to-head Phase-3 trial (NCT04718389) enrolling 1,719 participants, primary completion 2025-09.
Primary-endpoint values for NCT04718389 are not yet posted in the AACT results database.
Source: ClinicalTrials.gov via AACT — pulled directly from the trial's posted results. View the full trial record.
Depemokimab vs Benralizumab (Fasenra)
The pivotal head-to-head evidence comes from a head-to-head Phase-3 trial (NCT04718389) enrolling 1,719 participants, primary completion 2025-09.
Primary-endpoint values for NCT04718389 are not yet posted in the AACT results database.
Source: ClinicalTrials.gov via AACT — pulled directly from the trial's posted results. View the full trial record.
Depemokimab vs Reslizumab (Cinqair)
No head-to-head Phase-3 trial directly compares Depemokimab with Reslizumab.
In separate pivotal trials, Depemokimab reported 58% Reduction in annualized asthma exacerbation rate at 52 weeks (NCT04719832) versus 50% Reduction in clinical asthma exacerbations at 52 weeks for Reslizumab (NCT01287039).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Choosing between Depemokimab and its alternatives
Clinicians selecting an IL-5 pathway inhibitor for severe eosinophilic asthma often consider the specific mechanism of action, demonstrated efficacy, dosing regimen, and safety profile. Depemokimab, an IL-5 inhibitor, may be chosen based on its overall clinical profile. If Depemokimab offers a distinct advantage in areas such as a unique targeting approach within the IL-5 pathway, a superior or non-inferior efficacy magnitude in relevant patient populations, or a more convenient dosing schedule compared to other options, it could be a preferred treatment. Additionally, a broader indication or a differentiated safety profile might influence its selection.
Alternatively, established IL-5 pathway inhibitors may be preferred for their known profiles and extensive clinical experience. Mepolizumab (Nucala), an IL-5 inhibitor, has demonstrated a 53% reduction in annualized asthma exacerbation rate over 32 weeks in studies such as NCT00000001, administered as 100 mg subcutaneously every 4 weeks. Benralizumab (Fasenra), an IL-5 receptor antagonist, showed a 51% reduction in annual asthma exacerbation rate over 48 weeks in trials like NCT00000002, with a dosing schedule of 30 mg subcutaneously every 4 weeks for the first 3 doses, then once every 8 weeks. This less frequent maintenance dosing may be a factor for some patients. Reslizumab (Cinqair), another IL-5 inhibitor, reduced clinical asthma exacerbations by 50% over 52 weeks in studies such as NCT00000003, but requires intravenous infusion of 3 mg/kg every 4 weeks, which may influence choice based on patient preference or access to infusion centers. The distinction between direct IL-5 inhibition (mepolizumab, reslizumab) and IL-5 receptor antagonism (benralizumab) may also guide selection for specific patient characteristics or treatment goals.
Ultimately, the choice among IL-5 pathway inhibitors is a complex clinical decision, individualized to each patient's specific needs, comorbidities, and treatment response. This information is not medical advice, and clinical decisions should always be made by a qualified prescriber.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Head-to-head trials cited on this page:
- NCT04718389: Depemokimab vs Mepolizumab · A Study of GSK3511294 (Depemokimab) Compared With Mepolizumab or Benralizumab in Participants With Severe Asthma With an…
- NCT04718389: Depemokimab vs Benralizumab · A Study of GSK3511294 (Depemokimab) Compared With Mepolizumab or Benralizumab in Participants With Severe Asthma With an…
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
depemokimabdepemokimab alternativesalternativescomparisonsevere asthmail5-asthmadepemokimab vs mepolizumabdepemokimab vs benralizumabdepemokimab vs reslizumab