Opakalim is a Kv7.2/Kv7.3 potassium channel activator, representing a targeted approach within its drug class. This page provides a comparison of Opakalim with other antiepileptic drugs, including Lamotrigine (Lamictal), Levetiracetam (Keppra), and Topiramate (Topamax), highlighting differences in their mechanisms and clinical profiles.
Opakalim Alternatives: How It Compares to Other Kv7 Openers
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 0/7 curated
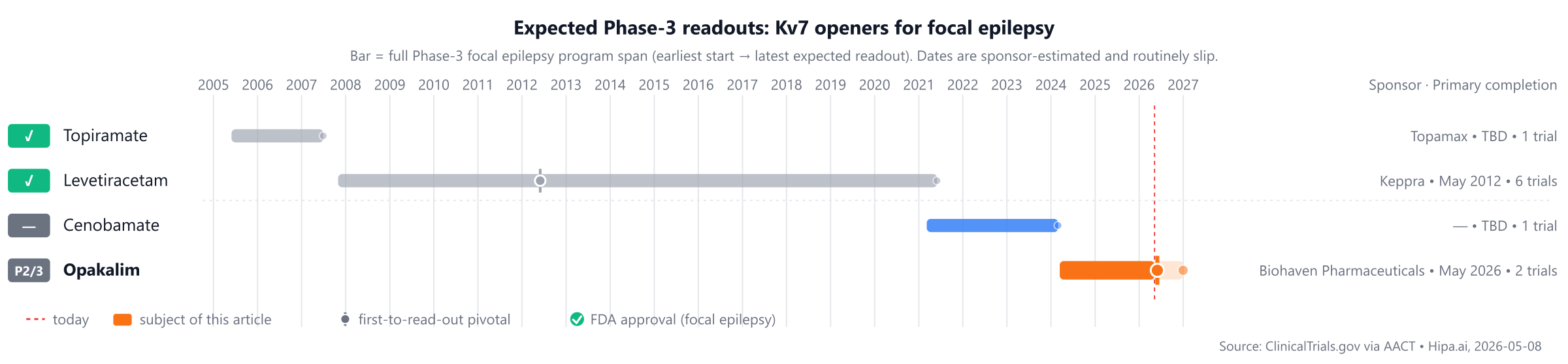
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-08Download chart as PNG
{kind=link}
The competitive landscape features long-approved treatments like Lamictal (Lamotrigine, approved 1994) and Topamax (Topiramate, approved 1996), while Opakalim is not yet approved. Several pipeline drugs, including Cenobamate, Valproate, and Azetukalner, are currently in Phase 3, with potential market entry approximately 1-2 years away.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Opakalim | Kv7.2/Kv7.3 potassium channel activator | — | Oral, once daily | Pipeline | — | — |
| Lamotrigine (Lamictal) | Sodium channel blocker | focal epilepsy, Lennox-Gastaut syndrome, bipolar I disorder, +1 more | Highly individualized based on indication, patient age, and concomitant medications (especially valproate or enzyme-inducing antiepileptic drugs). Requires a slow, multi-week dose titration to minimize the risk of serious skin rashes (e.g., Stevens-Johnson syndrome). Typical adult maintenance dose for epilepsy ranges from 100 mg to 400 mg daily. | 1994 | — | $150 |
| Topiramate (Topamax) | Anticonvulsant | Focal epilepsy, Primary generalized tonic-clonic seizures, Lennox-Gastaut syndrome, +1 more | 25 mg to 400 mg daily in two divided doses | 1996 | — | — |
| Levetiracetam (Keppra) | SV2A ligand | focal epilepsy, myoclonic seizures, primary generalized tonic-clonic seizures | 1000 mg/day initially (500 mg twice daily); may increase by 1000 mg/day every 2 weeks up to a maximum of 3000 mg/day. | 1999 | — | $150 |
| Cenobamate | — | — | — | Pipeline | — | — |
| Valproate | — | — | — | Pipeline | — | — |
| Azetukalner | Kv7 potassium channel opener | — | Once daily | Pipeline | Median percent reduction in monthly focal seizure frequency: 53.2% @ 12 weeks | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Median % reduction in seizure frequency; cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for focal epilepsy specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Opakalim vs Lamotrigine (Lamictal)
No head-to-head Phase-3 trial directly compares Opakalim with Lamotrigine.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Opakalim vs Levetiracetam (Keppra)
No head-to-head Phase-3 trial directly compares Opakalim with Levetiracetam.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Opakalim vs Topiramate (Topamax)
No head-to-head Phase-3 trial directly compares Opakalim with Topiramate.
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Several investigational alternatives are also in development, though with different mechanisms of action compared to Opakalim. Cenobamate (sponsor unknown) has been evaluated in Phase 3 studies, such as NCT01630545. Another agent, Valproate (sponsor unknown), has also been the subject of Phase 3 trials, including NCT00001642. These agents are approximately 1-2 years behind Opakalim in their development timelines.
Choosing between Opakalim and its alternatives
Opakalim, a Kv7.2/Kv7.3 potassium channel activator, offers a distinct mechanism of action compared to established antiepileptic drugs. This novel approach may be considered for patients who have not responded adequately to agents targeting other pathways. While specific efficacy data are not provided here, its unique mechanism could position it as a valuable option, particularly given the dosing complexities associated with some alternatives. For instance, lamotrigine requires a slow, multi-week dose titration to mitigate the risk of serious skin rashes, and both levetiracetam and topiramate also involve dose escalation phases to reach maintenance doses.
Conversely, clinicians may opt for alternatives such as lamotrigine (Lamictal), levetiracetam (Keppra), or topiramate (Topamax) due to their longer clinical track records and potentially lower cost, as they are well-established treatments. Lamotrigine, a sodium channel blocker, is highly individualized in its dosing and requires careful titration to minimize the risk of serious skin rashes, including Stevens-Johnson syndrome. Levetiracetam, an SV2A ligand, typically starts at 1000 mg/day and can be increased up to 3000 mg/day. Topiramate, another anticonvulsant, is dosed from 25 mg to 400 mg daily. These agents offer different mechanisms of action which may be preferred for specific patient profiles or comorbidities. This information is not medical advice; clinical decisions belong with the prescriber.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
opakalimopakalim alternativesalternativescomparisonfocal epilepsykv7-focal-epilepsyopakalim vs cenobamateopakalim vs lamotrigineopakalim vs levetiracetamopakalim vs topiramateopakalim vs valproate