Amivantamab is an EGFR/MET bispecific antibody approved for locally advanced or metastatic non-small cell lung cancer with specific EGFR mutations. This page compares its profile with other EGFR-targeted therapies, including Osimertinib (Tagrisso), Lazertinib (Lazcluze), and Erlotinib (Tarceva). Its unique dual targeting of both EGFR and MET pathways offers a distinct therapeutic strategy.
Amivantamab Alternatives: How It Compares to Other EGFR and MET Inhibitors
Hipa.ai Research · Source: ClinicalTrials.gov / AACT · Last updated: Limited data · 0/6 curated
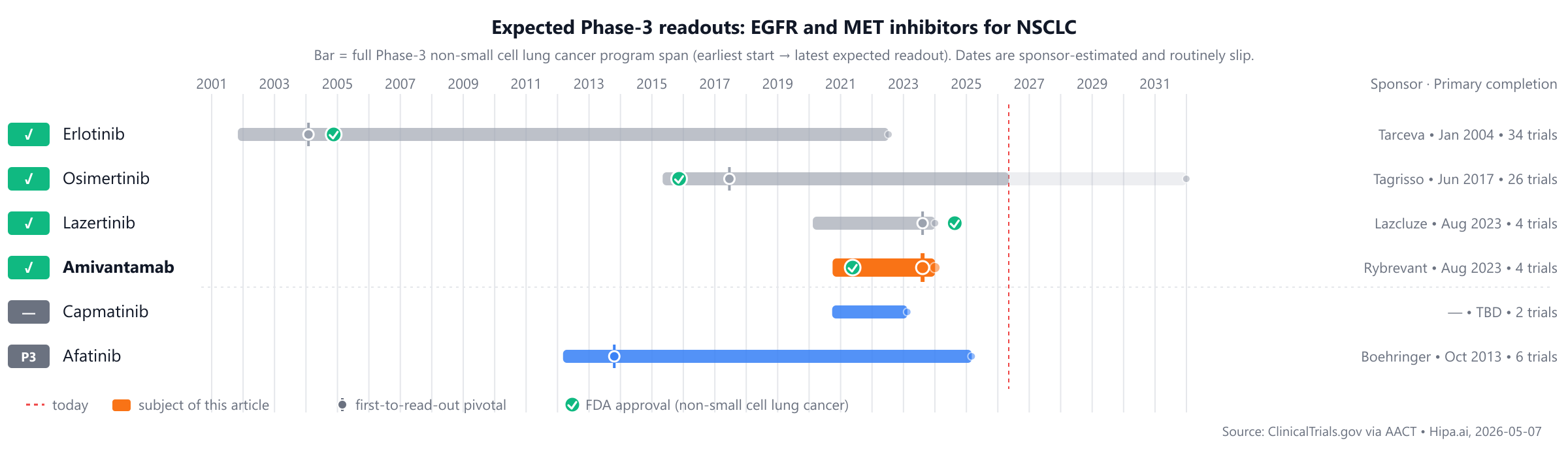
Source: ClinicalTrials.gov via AACT · Hipa.ai, 2026-05-07Download chart as PNG
{kind=link}
Approved comparators include Erlotinib (Tarceva, 2004) and Osimertinib (Tagrisso, 2015), with Amivantamab approved in 2021. Pipeline candidates Afatinib and Capmatinib are currently in Phase 3, approximately 1-2 years behind.
Quick comparison table
| Drug | Class | Approved indications | Dosing | Year approved | Lead pivotal endpoint | Annual cost (rough) |
|---|---|---|---|---|---|---|
| Amivantamab (Rybrevant) | EGFR/MET bispecific antibody | Locally advanced or metastatic non-small cell lung cancer (NSCLC) with EGFR exon 20 insertion mutations, Locally advanced or metastatic non-small cell lung cancer (NSCLC) with EGFR exon 19 deletions or exon 21 L858R substitution mutations | 1050 mg (<80 kg) or 1400 mg (≥80 kg) IV weekly for 4 weeks, then every 2 to 3 weeks; or 1600 mg (<80 kg) or 2240 mg (≥80 kg) SC weekly for 4 weeks, then every 2 to 4 weeks | 2021 | 23.7months @ median | $350k |
| Erlotinib (Tarceva) | EGFR inhibitor | non-small cell lung cancer, pancreatic cancer | 150 mg orally once daily for non-small cell lung cancer; 100 mg orally once daily for pancreatic cancer | 2004 | OS: 6.7months @ median | — |
| Osimertinib (Tagrisso) | EGFR tyrosine kinase inhibitor | Metastatic EGFR T790M mutation-positive non-small cell lung cancer, First-line metastatic EGFR-mutated non-small cell lung cancer, Adjuvant treatment of early-stage EGFR-mutated non-small cell lung cancer, +2 more | 80 mg orally once daily | 2015 | median progression-free survival: 18.9months @ overall | $216k |
| Lazertinib (Lazcluze) | EGFR tyrosine kinase inhibitor | Non-small cell lung cancer | 240 mg orally once daily | 2024 | 23.7months @ median | — |
| Afatinib | — | — | — | Pipeline | — | — |
| Capmatinib | — | — | — | Pipeline | — | — |
Cost estimates are list-price approximations and do not reflect rebates, formulary tier, or out-of-pocket costs after benefits. The class-typical lead-pivotal endpoint here is Progression-Free Survival (PFS); cells render each drug's actual pivotal endpoint, which may differ. The "Year approved" column shows the FDA approval year for non-small cell lung cancer specifically — drugs approved for other indications first appear with their this-indication date, or as Pipeline if not yet approved for this indication. Cross-trial comparisons can mislead — head-to-head Phase-3 data (when present) is below.
Amivantamab vs Osimertinib (Tagrisso)
The pivotal head-to-head evidence comes from a head-to-head Phase-3 trial (NCT04487080) enrolling 1,074 participants, primary completion 2023-08.
Progression-Free Survival (PFS) According to Response Evaluation Criteria in Solid Tumors (RECIST) Version 1.1 as Assessed by Blinded Independent Central Review (BICR): Active Comparator: Arm B (Double-blind): Osimertinib+Placebo Matching Lazertinib 16.59 Months; Experimental: Arm A (Open-label): Amivantamab + Lazertinib 23.72 Months; Experimental: Arm C (Double-blind): Lazertinib+Placebo Matching Osimertinib 18.46 Months
Source: ClinicalTrials.gov via AACT — pulled directly from the trial's posted results. View the full trial record.
Amivantamab vs Lazertinib (Lazcluze)
The pivotal head-to-head evidence comes from a head-to-head Phase-3 trial (NCT04487080) enrolling 1,074 participants, primary completion 2023-08.
Progression-Free Survival (PFS) According to Response Evaluation Criteria in Solid Tumors (RECIST) Version 1.1 as Assessed by Blinded Independent Central Review (BICR): Active Comparator: Arm B (Double-blind): Osimertinib+Placebo Matching Lazertinib 16.59 Months; Experimental: Arm A (Open-label): Amivantamab + Lazertinib 23.72 Months; Experimental: Arm C (Double-blind): Lazertinib+Placebo Matching Osimertinib 18.46 Months
Source: ClinicalTrials.gov via AACT — pulled directly from the trial's posted results. View the full trial record.
Amivantamab vs Erlotinib (Tarceva)
No head-to-head Phase-3 trial directly compares Amivantamab with Erlotinib.
In separate pivotal trials, Amivantamab reported 23.7months Progression-Free Survival (PFS) at median (NCT04487080) versus 6.7months OS at median for Erlotinib (NCT00036647).
Cross-trial caveat: the two drugs were tested in different patient populations at different time points. Cross-trial comparisons of response rates can mislead — the only rigorous comparison is a head-to-head randomized trial.
Pipeline alternatives
Among investigational agents in active Phase 3 development, Afatinib from Boehringer Ingelheim is undergoing evaluation, with its lead trial identified as NCT01523587. This agent functions as an irreversible ErbB family blocker, representing a distinct mechanism compared to Amivantamab, which is an EGFR-MET bispecific antibody. Additionally, Capmatinib, for which the sponsor is not specified in this context, is also in Phase 3 development, targeting the MET pathway. Both Afatinib and Capmatinib offer alternative therapeutic strategies by inhibiting pathways that are also targeted by Amivantamab.
Choosing between Amivantamab and its alternatives
When considering treatment options for patients with specific mutations, Amivantamab, an EGFR and MET bispecific antibody, offers a distinct mechanism of action compared to EGFR tyrosine kinase inhibitors (TKIs). This bispecific approach may be considered when a broader inhibition strategy targeting both pathways is deemed beneficial. While specific comparative efficacy data for Amivantamab versus the listed EGFR TKIs is not provided here, its unique dual-target binding could represent a different therapeutic avenue for certain patient profiles.
Conversely, established EGFR TKIs like Osimertinib, Lazertinib, and Erlotinib may be preferred based on their extensive clinical experience and well-characterized profiles. Osimertinib (Tagrisso) has demonstrated a median progression-free survival of 18.9 months with an 80 mg oral once-daily dose. Lazertinib (Lazcluze) showed a median progression-free survival of 23.7 months at a 240 mg oral once-daily dose. Erlotinib (Tarceva) has a median overall survival of 6.7 months, typically dosed at 150 mg or 100 mg orally once daily depending on the indication. These agents, as single-target EGFR inhibitors, may offer a different balance of efficacy, tolerability, and potentially cost considerations, depending on individual patient characteristics and treatment goals. The choice between a bispecific antibody and a TKI often involves a comprehensive assessment of the patient's specific mutation status, prior treatments, and overall clinical picture.
This information is for educational purposes only and does not constitute medical advice. Clinical decisions should always be made by a qualified healthcare professional in consultation with the patient.
Sources and methodology
Trial data was pulled from the ClinicalTrials.gov registry via the AACT relational mirror maintained by the Clinical Trials Transformation Initiative. AACT data freshness: .
Head-to-head trials cited on this page:
- NCT04487080: Amivantamab vs Osimertinib · A Study of Amivantamab and Lazertinib Combination Therapy Versus Osimertinib in Locally Advanced or Metastatic Non-Small…
- NCT04487080: Amivantamab vs Lazertinib · A Study of Amivantamab and Lazertinib Combination Therapy Versus Osimertinib in Locally Advanced or Metastatic Non-Small…
Cross-trial comparison limitations:drugs without a direct head-to-head trial are compared using each drug's own pivotal trial. These trials enrolled different patient populations at different time points and used different statistical analysis sets. Cross-trial response-rate differences should not be interpreted as proof that one drug is more effective than another.
Related drug pages on Hipa.ai
Not medical advice. This page summarizes publicly-reported clinical trial data for informational purposes. Treatment decisions belong with a qualified prescribing clinician who knows your medical history. Drug approvals, dosing, and safety profiles change over time — always confirm with the current FDA prescribing information.
amivantamabamivantamab alternativesalternativescomparisonnon-small cell lung canceregfr-met-nsclcamivantamab vs osimertinibamivantamab vs lazertinibamivantamab vs afatinibamivantamab vs erlotinibamivantamab vs capmatinib